Decreased serum ferritin and vitamin D levels in patients with recurrent aphthous stomatitis

1Ufuk University School of Medicine, Department of Dermatology, Ankara, Turkey; 2General Directorate of Public Health, Department of Infectious Diseases, Ankara, Turkey
Corresponding author: Dr. Funda Tamer, E-mail: fundatmr@yahoo.com
Submission: 18.11.2018; Acceptance: 27.01.2019
DOI: 10.7241/ourd.20193.1
Cite this article: Tamer F, Avci E. Decreased serum ferritin and vitamin D levels in patients with recurrent aphthous stomatitis. Our Dermatol Online. 2019;10(3):229-233.
Citation tools:
BibTex | CSV | RIS | refer/BiblX | Endnote XML | Wikipedia Citation Templates
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Background: Recurrent aphthous stomatitis is the most common ulcerative disease of the oral mucosa. Several predisposing factors like oral microbial flora, stress, viral infections, vitamin and mineral deficiencies have been associated with the disease. However, the etiopathogenesis of recurrent aphthous stomatitis remains unknown.
Material and Methods: The study included 20 patients with recurrent aphthous stomatitis and 20 healthy individuals within the control group. Complete blood count, serum levels of ferritin, folate, vitamin B12, zinc, 25-hydroxyvitamin D, herpes simplex virus type-1 IgG and herpes simplex virus type-2 IgG were evaluated in each participant.
Results: White blood cell count, platelet count, mean platelet volume, mean serum levels of hemoglobin, folate, vitamin B12 and zinc were statistically similar in patients and healthy individuals. However, the mean serum ferritin level was significantly lower in patients (26.5±25.5 ng/mL) compared to healthy individuals (42±30 ng/mL) (p=0.04). The mean serum 25-hydroxyvitamin D level was significantly lower in patients (13.6±6.5 ng/mL) compared to healthy individuals (20.9±10 ng/mL) (p=0.01). No significant difference has been observed between two groups in the frequency of positive serum herpes simplex virus type-1 IgG and herpes simplex virus type-2 IgG levels.
Conclusions: No association has been observed between recurrent aphthous stomatitis and white blood cell count, mean platelet volume, serum levels of hemoglobin, folate, vitamin B12, zinc, herpes simplex virus type-1 IgG and herpes simplex virus type-2 IgG. However, decreased serum levels of ferritin and 25-hydroxyvitamin D were more prevalent in patients with recurrent aphthous stomatitis compared to healthy individuals.
Key words:Aphthous, Ferritin, Recurrent, Stomatitis, Vitamin D
INTRODUCTION
Recurrent aphthous stomatitis is the most common inflammatory disease of the oral mucosa. It is characterized by painful round ulcers with pseudomembranous center and erythematous borders [1,2]. The prevalence of the disease is 0.5% to 75% all over the world. Recurrent aphthous stomatitis is more common in women than in men. The ulcers usually begin during the second decade of life [1]. Recurrent aphthous stomatitis is classified into three clinical types; minor, major, and herpetiform ulcers [2]. Most of the patients (>85%) with recurrent aphthous stomatitis present with minor ulcers that have a diameter less than 1 cm [2]. Major ulcers (Sutton’s disease) have a diameter greater than 1 cm and they can persist for weeks [2,3]. Herpetiform type presents as multiple, small ulcers with 1-2 mm in size, that may heal with scarring [1].
The etiopathogenesis of recurrent aphthous stomatitis remains unknown. However, several predisposing factors have been associated with the disease. Genetic predisposition, iron, vitamin B12 and folic acid deficiencies, nonsteroidal anti-inflammatory drugs, angiotensin converting enzyme inhibitors, gluten sensitive enteropathy, inflammatory bowel disease, stress, trauma to oral mucosa like dental procedures, Helicobacter pylori and viral infections have been implicated in the development of recurrent aphthous stomatitis [4].
The differential diagnosis should include chickenpox, erythema multiforme, erosive lichen planus, Riga-Fede disease, pemphigus vulgaris and pemphigoid [5]. Treatment of recurrent aphthous stomatitis can be difficult particularly in severe cases [6]. It is crucial to rule out an underlying systemic disorder in the management of disease. However, most of the patients are healthy except for painful oral ulcers [7]. Topical therapies include chlorhexidine rinse, antibiotics like doxycycline and minocyclin, diclofenac, benzocaine, lidocaine and corticosteroids. Furthermore, penicillin G, rifampin, dapsone, zinc, pentoxifylline, thalidomide, colchicine and ascorbic acid have been used in the management of recurrent aphthous stomatitis [6].
MATERIALS AND METHODS
The study included 20 patients with recurrent aphthous stomatitis and 20 healthy individuals within the control group. Medical records of the participants were reviewed retrospectively between January 2018 and September 2018. Laboratory tests including complete blood count, serum levels of ferritin, folate, vitamin B12, zinc, 25-hydroxyvitamin D (25(OH)D), herpes simplex virus type-1 (HSV1) IgG and herpes simplex virus type-2 (HSV2) IgG were evaluated in each participant. The exclusion criteria were pregnancy, immunosuppression, malignancy, inflammatory bowel disease, diet restrictions, vitamin and mineral supplements.
Data were represented as mean ± standard deviation or median for quantitative variables; counts and percentage for categorical variables. Differences between two groups were tested with Mann Whitney U test for continuous variables and chi-square or Fisher exact tests as appropriate for categorical variables. The data were analyzed using SPSS 20.0 Statistical Package Program.
RESULTS
The study included 20 patients (15 female, 5 male) with recurrent aphthous stomatitis and 20 healthy individuals (14 female, 6 male) within the control group. The mean age of the patients was 34±12.3 (range: 18-58). The mean age of the healthy individuals was 33.9±13.4 (range: 18-60) (p=1). The mean disease duration was 24.6±32.9 months (range: 1-120 months). Three (15%) patients had at least one first-degree family member who suffered from recurrent aphthous stomatitis.
The mean hemoglobin level of the patients and healthy individuals were 13.6±1.5 g/dL and 14.3±1.2 g/dL, respectively (p=0.1) (normal range: 11.7-17 g/dL). Two (10%) patients had decreased serum hemoglobin levels, while all the healthy individuals had normal serum hemoglobin levels (p=0.4). The mean white blood cell count of the patients and healthy individuals were 7.3±1.6 103/µL and 6.7±1.3 103/µL, respectively (p=0.3) (normal range: 4.2-10.2 103/µL). All the participants had normal serum white blood cell count. The mean platelet count of the patients and healthy individuals were 255.4±68.5 103/µL and 252.4±54.5 103/µL, respectively (p=0.7) (normal range: 142-450 103/µL). One (5%) patient had low platelet count, while all the healthy individuals had normal platelet counts (p=1). The mean platelet volume of the patients and healthy individuals were 7.888±1.4 fL and 7.913±0.9 fL, respectively (p=0.7) (normal range: 6.4-11 fL). Three (15%) patients and one (5%) healthy individual had low mean platelet volume. Increased mean platelet volume was observed only in one (5%) patient (p=0.3).
The mean serum ferritin level of the patients and healthy individuals were 26.5±25.5 ng/mL and 42±30 ng/mL, respectively (p=0.04) (normal range: 10-204 ng/mL). Low serum ferritin levels were observed in 6 (30%) patients and 2 (10%) healthy individuals (p=0.2) (Fig. 1). The mean serum folate level of the patients and healthy individuals were 5.7±1.8 µg/L and 6.6±2.2 µg/L, respectively (p=0.1) (normal range: 3.1-20 µg/L). All the participants had normal serum folate levels. The mean serum vitamin B12 level of the patients and healthy individuals were 343.7±171.9 pg/mL and 281.6±93.9 pg/ mL, respectively (p=0.2) (normal range: 190-880 pg/mL). Four (20%) patients had low serum vitamin B12 levels, while 3 (15%) healthy individuals had low serum vitamin B12 levels (p=1). The mean serum zinc level of the patients and healthy individuals were 78.8±14.4 µg/dL and 85.3±15.9 µg/L, respectively (p=0.1) (normal range: 60-150 µg/dL). All the participants had normal serum zinc levels. The mean serum 25(OH)D level of the patients and healthy individuals were 13.6±6.5 ng/mL and 20.9±10 ng/mL, respectively (p=0.01) (normal range: 20-60 ng/mL). Fourteen (70%) patients had decreased serum 25(OH)D levels, while 9 (45%) healthy individuals had decreased serum 25(OH)D levels (p=0.2) (Fig. 2).
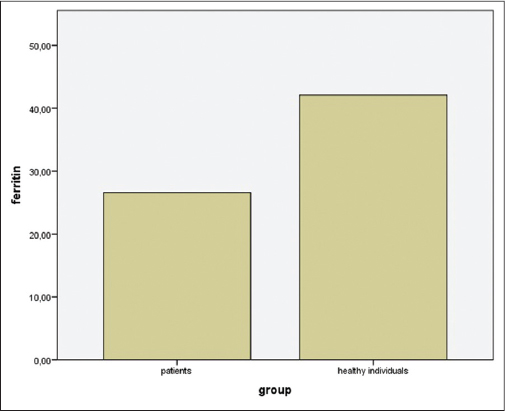 |
Figure 1: The mean serum ferritin level of the patients (26.5±25.5 ng/mL) was significantly lower compared to healthy individuals (42±30 ng/mL) (p=0.04). |
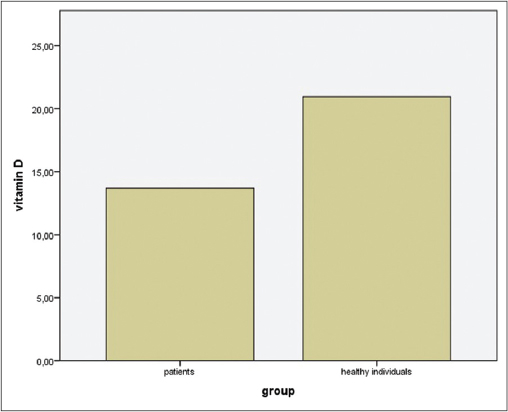 |
Figure 2: The mean serum 25(OH)D level of the patients (13.6±6.5 ng/mL) was significantly lower compared to healthy individuals (20.9±10 ng/mL) (p=0.01). |
The mean serum HSV1 IgG level of the patients and healthy individuals were 52.6±72.4 RU/mL and 80.8±83.9 RU/mL, respectively (p=0.4) (range: negative<16, positive>22 RU/mL). Positive serum HSV1 IgG levels were observed in eleven (55%) patients and in 10 (50%) healthy individuals (p=1). The mean serum HSV2 IgG level of the patients and healthy individuals were 10.5±34.3 RU/mL and 2.6±2.9 RU/mL, respectively (p=0.4) (range: negative<16, positive>22 RU/mL). Positive serum HSV2 IgG level was observed in one (5%) patient. None of the healthy individuals had positive serum HSV2 IgG level (p=1).
DISCUSSION
Despite being the most common ulcerative disease of the oral mucosa, the etiology of recurrent aphthous stomatitis has not been clearly identified yet. Therefore, current treatment options are usually aim to reduce symptoms [8]. Impaired mucosal barrier function, stress, oral microbial flora including Streptococcus sanguinis and Streptococcus mitis, Helicobacter pylori infection, diet, allergies, vitamin and mineral deficiencies, hematological parameters like ferritin, hemoglobin and hematocrit have been associated with recurrent aphthous stomatitis. Moreover, high levels of erythrocyte sedimentation rate, mean platelet volume, white blood cells, neutrophils and homocysteine have been reported in patients with recurrent aphthous stomatitis [8].
Sun et al. investigated hemoglobin, iron, vitamin B12, folic acid, and homocysteine concentrations in patients with recurrent aphthous stomatitis and in healthy controls. Elevated homocysteine levels and decreased levels of hemoglobin, iron, vitamin B12 and folic acid were significantly more common in patients than in control group [9]. Compilato et al. evaluated hematological deficiencies in 32 patients with recurrent aphthous stomatitis and in 29 healthy controls. Serum iron, folic acid and vitamin B12 deficiencies were significantly more common in patient group than in healthy individuals [10]. Chen et al. reported high rates of hemoglobin, ferritin, folic acid and vitamin B12 deficiencies in patients with recurrent aphthous stomatitis [11]. Similarly, Lopez-Jornet et al. reported that iron, folic acid, and vitamin B12 deficiencies were more frequent in patients with recurrent aphthous stomatitis compared to healthy controls [12].
Within this study, the mean serum hemoglobin level was lower in patients (13.6±1.5 g/dL) compared to healthy individuals (14.3±1.2 g/dL). However, no statistically significant difference has been observed in hemoglobin levels between two groups (p=0.1). White blood cell count, platelet count and mean platelet volume were similar in patients with recurrent aphthous stomatitis and healthy individuals within the control group. The mean serum ferritin level was significantly lower in patients (26.5±25.5 ng/mL) compared to healthy individuals (42±30 ng/mL) (p=0.04). The mean serum folate level was lower in patients (5.7±1.8 µg/L) than in control group (6.6±2.2 µg/L). However, no statistically significant difference has been observed in folate levels between two groups (p=0.1). In contrast, mean serum vitamin B12 levels were higher in patients (343.7±171.9 pg/mL) compared to healthy individuals (281.6±93.9 pg/ mL). However, no statistically significant difference has been observed in vitamin B12 levels between two groups (p=0.2).
Association between serum zinc concentration and recurrent aphthous stomatitis remains controversial. Ślebioda et al. detected no significant difference in serum zinc levels between patients with recurrent aphthous stomatitis and healthy controls, while Ozler reported a distinct association between zinc deficiency and recurrent aphthous stomatitis [13,14].
Within this study, serum zinc levels of the participants were all in normal limits. Patients with recurrent aphthous stomatitis had lower serum zinc levels (78.8±14.4 µg/dL) compared to healthy individuals (85.3±15.9 µg/L). However, no statistically significant difference has been observed in zinc levels between two groups (p=0.1).
Low serum vitamin D level has been implicated as a facilitating factor in the development of recurrent aphthous stomatitis. Oztekin et al. reported significantly lower serum vitamin D levels in patients with recurrent aphthous stomatitis compared to healthy individuals [15]. In contrast, Krawiecka et al. reported similar serum vitamin D levels in patients with recurrent aphthous stomatitis and healthy controls [16].
Within this study, the mean serum 25(OH)D level was significantly lower in patients (13.6±6.5 ng/mL) than in control group (20.9±10 ng/mL) (p=0.01). Vitamin D deficiency was detected in 70% of the patients with recurrent aphthous stomatitis.
It has been suggested that the human herpesviruses (HHVs) may play role in the development of recurrent aphthous stomatitis. However, Brice et al. examined the members of the HHV family including HSV1, HSV2, varicella zoster virus, Epstein-Barr virus, cytomegalovirus, HHV-6, HHV-7 and HHV-8, in the oral mucosa of patients with recurrent aphthous stomatitis and control subjects. The frequency of detection of HHV DNA was not greater in the mucosa of patients than in controls [17]. In addition, Seoudi et al. reported no significant difference between HSV1 IgG and HSV2 IgG levels in patients with Behçet’s disease, recurrent aphthous stomatitis and healthy controls [18].
Within this study, a positive HSV1 IgG result was detected in 55% of the patients with recurrent aphthous stomatitis and in 50% of healthy individuals, whereas only one patient was HSV2 IgG positive. The results indicate no correlation between HSV and recurrent aphthous stomatitis.
In conclusion, this study revealed no association between recurrent aphthous stomatitis and mean platelet volume, white blood cell count, HSV1, HSV2, serum levels of hemoglobin, folate, vitamin B12 and zinc. However, decreased serum levels of ferritin and 25(OH)D were more prevalent in patients with recurrent aphthous stomatitis compared to healthy individuals. Therefore, we suggest that serum ferritin and 25(OH)D levels should be evaluated in all patients with recurrent aphthous stomatitis. Replacement therapies may be helpful in the management of the disease in cases with iron or vitamin D deficiency.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
REFERENCES
1. Mortazavi H, Safi Y, Baharvand M, Rahmani S. Diagnostic features of common oral ulcerative lesions:an updated decision tree. Int J Dent. 2016;2016:7278925.
2. Akintoye SO, Greenberg MS. Recurrent aphthous stomatitis. Dent Clin North Am. 2014;58:281-97.
3. Brzeziński P, Wollina U, Espinoza-Benavides L, Chang P, Mohamed M, Geller SA. Dermatology eponyms–sign–lexicon (S). Part II. Our Dermatol Online. 2018;9:470-7.
4. Cui RZ, Bruce AJ, Rogers RS 3rd. Recurrent aphthous stomatitis. Clin Dermatol. 2016;34:475-81.
5. Queiroz SIML, Silva MVAD, Medeiros AMC, Oliveira PT, Gurgel BCV, Silveira ÉJDD. Recurrent aphthous ulceration:an epidemiological study of etiological factors, treatment and differential diagnosis. An Bras Dermatol. 2018;93:341-6.
6. Edgar NR, Saleh D, Miller RA. Recurrent aphthous stomatitis:a review. J Clin Aesthet Dermatol. 2017;10:26-36.
7. Woo SB, Sonis ST. Recurrent aphthous ulcers:a review of diagnosis and treatment. J Am Dent Assoc. 1996;127:1202-13.
8. Saikaly SK, Saikaly TS, Saikaly LE. Recurrent aphthous ulceration:a review of potential causes and novel treatments. J Dermatolog Treat. 2018;29:542-52.
9. Sun A, Chen HM, Cheng SJ, Wang YP, Chang JY, Wu YC, et al. Significant association of deficiencies of hemoglobin, iron, vitamin B12, and folic acid and high homocysteine level with recurrent aphthous stomatitis. J Oral Pathol Med. 2015;44:300-5.
10. Compilato D, Carroccio A, Calvino F, Di Fede G, Campisi G. Haematological deficiencies in patients with recurrent aphthosis. J Eur Acad Dermatol Venereol. 2010;24:667-73.
11. Chen H, Sui Q, Chen Y, Ge L, Lin M. Impact of haematologic deficiencies on recurrent aphthous ulceration:a meta-analysis. Br Dent J. 2015;218:E8.
12. Lopez-Jornet P, Camacho-Alonso F, Martos N. Hematological study of patients with aphthous stomatitis. Int J Dermatol. 2014;53:159-63.
13. Ślebioda Z, Krawiecka E, Szponar E, Dorocka-Bobkowska B. Evaluation of serum zinc levels in patients with recurrent aphthous stomatitis (RAS). BMC Oral Health. 2017;17:158.
14. Ozler GS. Zinc deficiency in patients with recurrent aphthous stomatitis:a pilot study. J Laryngol Otol. 2014;128:531-3.
15. Öztekin A, Öztekin C. Vitamin D levels in patients with recurrent aphthous stomatitis. BMC Oral Health. 2018;18:186.
16. Krawiecka E, Ślebioda Z, Szponar E, Kowalska A, Dorocka-Bobkowska B. Vitamin D status in recurrent aphthous stomatitis. Postepy Dermatol Alergol. 2017;34:612-7.
17. Brice SL, Cook D, Leahy M, Huff JC, Weston WL. Examination of the oral mucosa and peripheral blood cells of patients with recurrent aphthous ulceration for human herpesvirus DNA. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:193-8.
18. Seoudi N, Bergmeier LA, Hagi-Pavli E, Bibby D, Fortune F. The seroprevalence and salivary shedding of herpesviruses in Behçet’s syndrome and recurrent aphthous stomatitis. J Oral Microbiol. 2015;7:27156.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-4157-5583 http://orcid.org/0000-0003-4157-5583
|

Comments are closed.