CREST syndrome-A clinical and dermoscopic perspective
Alin Laurentiu Tatu
Faculty of Medicine and Pharmacy, University ,,Dunarea de Jos “, Galati, Romania
Corresponding author: Alin Laurentiu Tatu, MD PhD, E-mail: dralin_tatu@yahoo.com
Submission: 19.03.2017; Acceptance: 28.03.2017
DOI: 10.7241/ourd.2017e.8
How to cite this article: Tatu AL. CREST syndrome-A clinical and dermoscopic perspective. Our Dermatol Online. 2017;8(1e):e9.
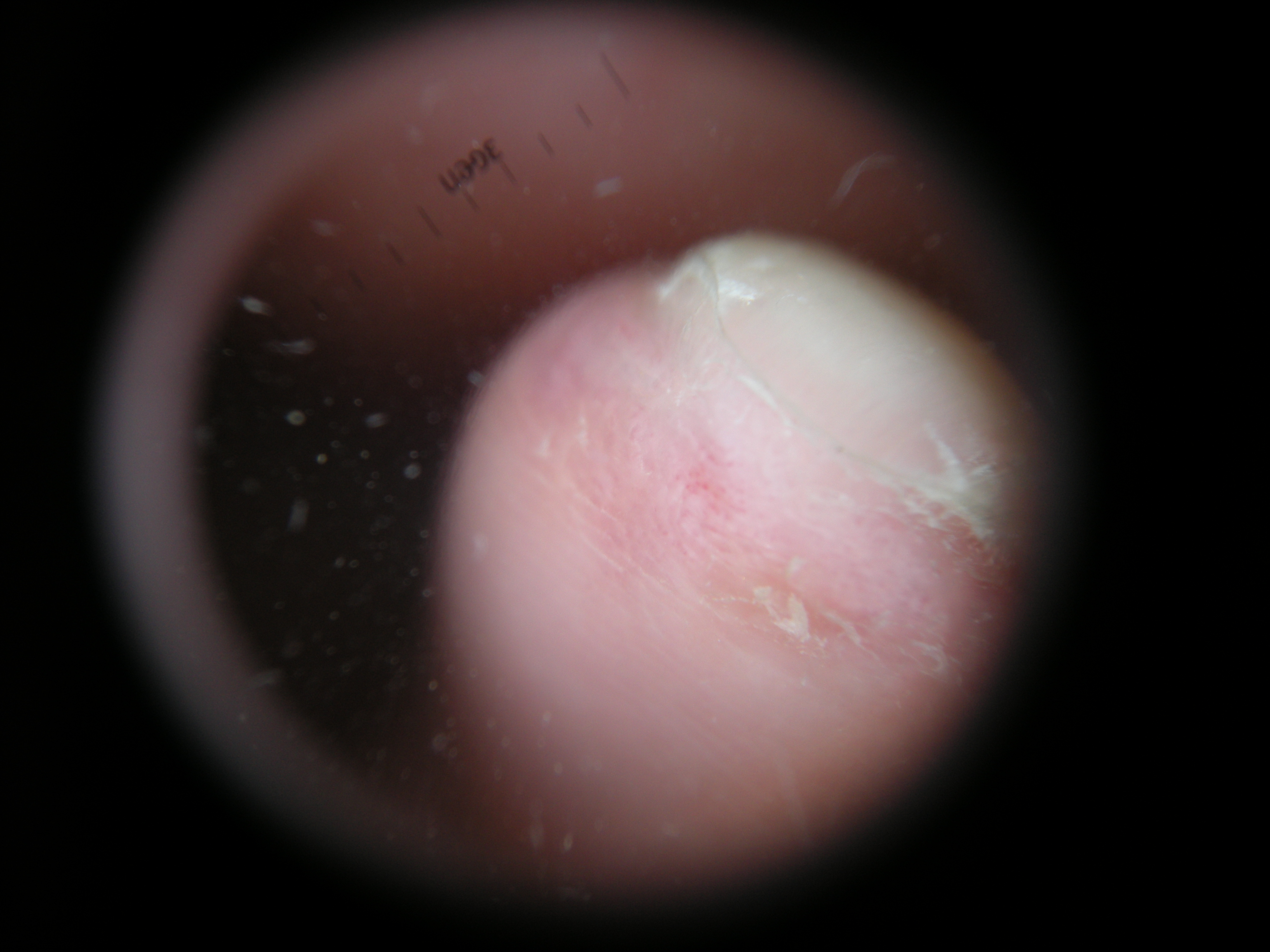
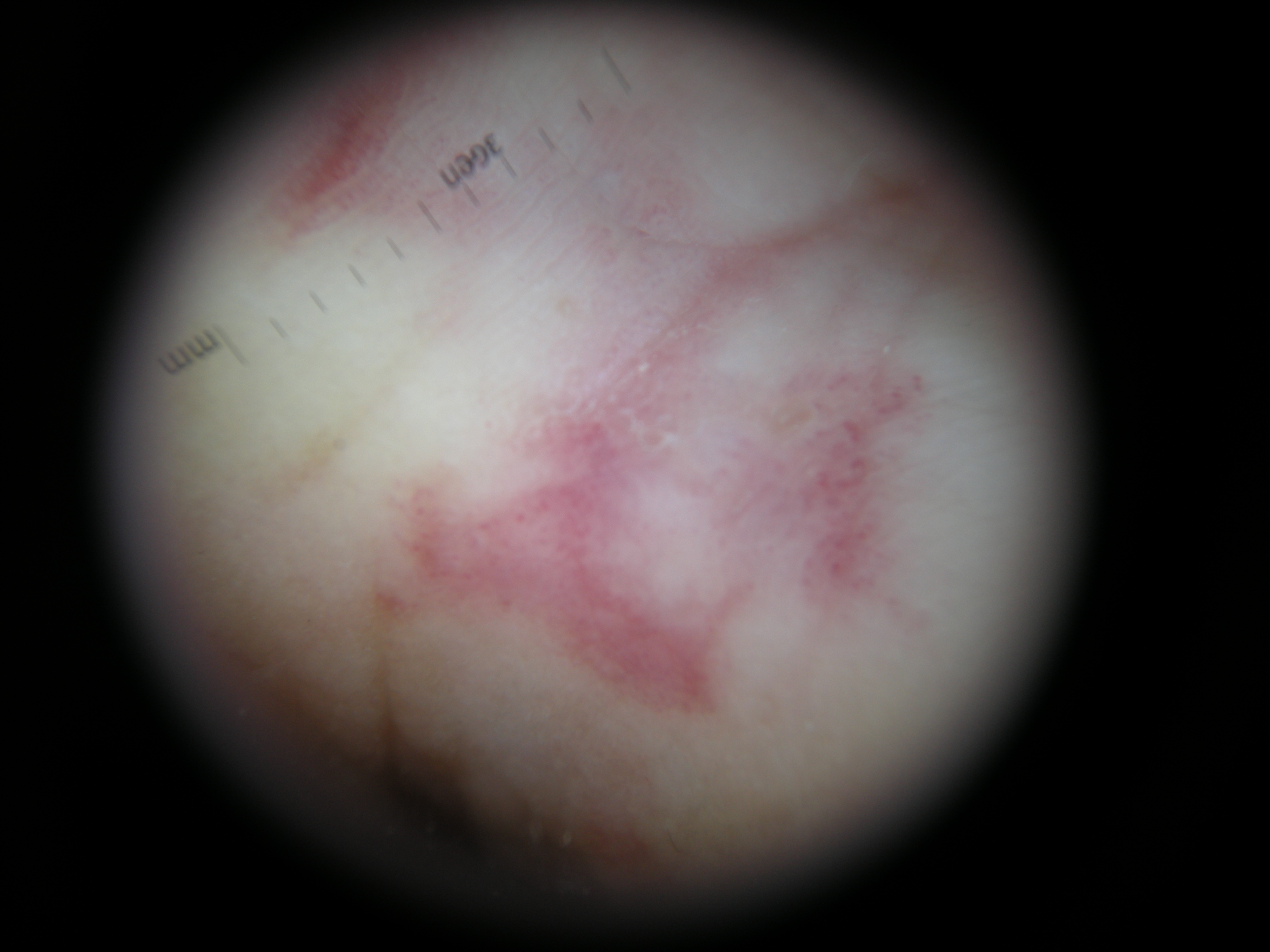
A 59-year-old woman was diagnosed with scleroderma. Five years later she developed swallowing difficulties, constipation, weight loss, arrhythmias and from rheumatology she was referred to dermatology for the skin changes. On examination there were skin nodules on the fingers from calcinosis, Reynaud’s phenomenon, sclerodactyly with ulcerations of the distal fingers (Figs. 1a and 1b) with a hardened skin on fingers, severe tightening of the facial skin with difficulties to open the mouth, dry mouth and eyes.

On the face and palms there were vissible telangiectasias (Figs. 2a and 2b) and loss of subcutaneous fat on her, trunk, upper limbs and face with movement limitations (Fig. 3). We diagnosed her condition as CREST syndrome. The skin treatment was empirically indicated: gentle skin cleansers, moisturizers, regular streching exercise with physical therapist, quit smoking, gloves wearing, laser surgery for telangiectasias. The dermatology and rheumatology follow –up was recommended.


Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.