A nodule on the breast: what’s your diagnosis?
Safa Idoudi 1, Mouna Korbi1, Mohamed Ben Rejeb1, Nouha Ben Abdeljelil2
1, Mouna Korbi1, Mohamed Ben Rejeb1, Nouha Ben Abdeljelil2
1Department of Dermatology, Fattouma Bourguiba University Hospital, Monastir, Tunisia; 2Department of Anapathology, Fattouma Bourguiba University Hospital, Monastir, Tunisia
Corresponding author: Dr. Safa Idoudi
Submission: 22.05.2020; Acceptance: 28.06.2020
DOI: 10.7241/ourd.2020e.81
Cite this article: IdIdoudi S, Korbi M, Rejeb MB, Abdeljelil NB. A nodule on the breast: what’s your diagnosis?. Our Dermatol Online. 2020;11(e):e81.1-e81.2.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
A 35-year-old healthy women presented with well-circumscribed purplish nodule of the right breast. The lesion was painless and had enlarged insidiously for more than 3 months. The patient reported no previous trauma or insect bite to the area involved. Physical examination revealed a dark reddish nodule, measuring about 1*1.5 cm with a cystic appearance (Fig. 1). There was neither ulceration nor crusting, and the dimple sign was negative.
 |
Figure 1: Dark reddish nodule, measuring about 1*1.5 cm with a cystic appearance of the right breast. |
Dermoscopic examination revealed homogeneous bluish purple pigmentation with a scaly surface and a central whitish area with fine shiny linear whitish structures surrounded by a delicate light brown pigment network (Fig. 2).
 |
Figure 2: Homogeneous bluish purple pigmentation with a scaly surface and a central whitish area with fine shiny linear whitish structures (grey circle) surrounded by a delicate light brown pigment network (black arrow). |
HISTOPATHOLOGY
Microscopic examination disclosed a dense dermal fibrohistiocytic infiltrate in a rich connective vascular stroma (Fig. 3) with a hemosiderin pigments deposition and dilated blood vessels (Fig. 4).
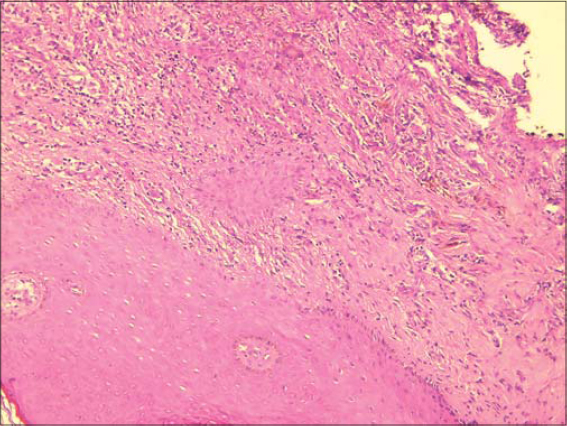 |
Figure 3: Dense dermal fibrohistiocytic infiltrate in a rich connective vascular stroma (HE* 100). |
 |
Figure 4: A hemosiderin pigments deposition and dilated blood vessels (HE*400). |
WHAT’S YOUR DIAGNOSIS?
Aneurysmal dermatofibroma (ADF)
Dermatofibroma is a benign dermal fibrohistiocytic tumor that manifests a variety of clinical, histopathological, and dermoscopic patterns. Aneurysmal dermatofibroma (ADF) is considered as one of the most atypical and rare variant of DF with reported incidence less than 2% of total cases [1]. It usually appears as a unique nodule of the lower extremities among middle-aged females. Commonly, of red to blue-black color and larger than typical DF [2]. Some dermatologists and dermatopathologists consider that ADF is probably an advanced stage in the development of haemosiderotic dermatofibroma [3]. Clinically, ADF may be misdiagnosed as nodular melanoma for the dark pigmentation and rapid growth of the tumor [4]. Histopathologically, ADF may be confused with other cutaneous tumors, especially hemangiomas, because of the presence of blood-filled tissue spaces, background vascularity, and abundant hemosiderin pigment and extravasated erythrocytes [5]. Thus, diagnosis is most of the time challenging. Dermoscopy of common DF have been widely described as a typical pattern with a central white scar-like patch and a delicate pigment network at the periphery [6]. Remarkably, there are very few reports describing dermoscopically the aneurysmal variant of DF. As reported by Zaballos et al [7], were found in our patient a homogeneous bluish purple pigmentation corresponding to prominent blood-filled spaces and a central whitish area with fine shiny linear whitish structures more likely to be caused by a pronounced fibrosis within the papillary dermis. The delicate light brown pigment network surrounding the tumor is related to the hyperpigmented rete ridges usually present at the edge of dermatofibromas. Kelati et al [8], reported a new dermoscopic description of this polymorphous tumor as a white ring around an ulceration associated with linear irregular vessels and dotted vessels. These findings were related to the histological presence of large and superficial bloodfilled spaces that may cause epidermal removal and ulceration surrounded by fibrosis. A rainbow pattern, typically described in Kaposi sarcoma has also been reported as a potent dermoscopic sign of ADF [9].
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
REFERENCES
1. Nabatanzi A, Male M, Qu XY, Li YQ, Meng X, Di WS, et al. Aneurysmal fibrous histiocytoma:clinicopathology analysis of 30 cases of a rare variant of cutaneous fibrohistiocytoma. Curr Med Sci. 2019;39:134-7.
2. Zaballos P, Llambrich A, Ara M, Olazaran Z, Malvehy J, Puig S. Dermoscopic findings of haemosiderotic and aneurysmal dermatofibroma:report of six patients. Br J Dermatol. 2006;154:24450.
3. Chang P, Monzón Quintana ML, Pacheco GC. Piloleiomiomas multiples. Our Dermatol Online. 2018;9:86-8.
4. Dheenadhayalan K, Srinivasan S, Bakthavatsalam S. An unusual misleading multiple nodules on the extremities –a case report. Our Dermatol Online. 2016;7:59-61.
5. Ben Rejeb S, Dhaoui A, Ben Ghachem D, Souissi A, Bellil K. Multiple eruptive dermatofibromas occuring in a patient under hemodialysis. Our Dermatol Online. 2016;7:412-4.
6. Zaballos P, Puig S, Llambrich A, Malvehy J. Dermoscopy of dermatofibromas:a prospective morphological study of 412 cases. Arch Dermatol. 2008;144:75–8
7. Zaballos P, Llambrich A, Ara M, Olazarán Z, Malvehy J, Puig S. Dermoscopic findings of haemosiderotic and aneurysmal dermatofibroma:report of six patients. Br J Dermatol. 2006;154:244–50.
8. Kelati A, Aqil N, Baybay H, Gallouj S, Mernissi FZ. Beyond classic dermoscopic patterns of dermatofibromas:a prospective research study. J Med Case Rep. 2017;11:266.
9. Padilla-Espana L, Fernandez-Canedo I, Blazquez-Sanchez N. Fast-growing pigmented nodular lesions. Actas Dermosifiliogr. 2015;106:505-6.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.