The effect of combined calcipotriol and betamethasone dipropionate ointment in the treatment of localized vitiligo
Igor Feszak1, Piotr Brzezinski 1,2, Mateusz Wityk3
1,2, Mateusz Wityk3
1Department of Dermatology, Voivodeship Specialist Hospital in Slupsk, Poland, 2Department of Physiotherapy and Medical Emergency, Faculty of Health Sciences, University Academy, Slupsk, Poland, 3Department of General and Oncological Surgery, Voivodeship Specialist Hospital in Slupsk, Poland
Citation tools:


Copyright information
© Our Dermatology Online 2023. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
Vitiligo is an autoimmune skin disease that attacks melanocytes and prevents them from producing melanin. This process manifests as depigmented spots of various shapes and sizes surrounded by a darker border without inflammation. The disease affects 0.5–2% of the world’s population, with no significant difference in terms of gender [1]. Hereditary, genetic, and environmental factors are believed to be the main contributors to the risk of vitiligo. The disease usually appears in patients before the age of 30 and even at younger ages among patients with a positive family history. Spontaneous regression of the disease is slow, and distal body parts, such as the hands and feet, are more resistant to repigmentation than other body parts. The disease is associated with a decrease in patients’ quality of life and may contribute to psychological disorders [2].
We report the case of a 62-year-old female who has had a vitiligo lesion on the right side of her forehead since she was 55 years old. She was diagnosed with vitiligo at the age of 57. The patient was treated with a combination of calcipotriol 0.005% and betamethasone dipropionate 0.05% in ointment form with a good response. Figure 1 shows the progress of treatment. We can see a change on the day before the beginning of treatment (Fig. 1a), followed by a noticeable onset of depigmentation on day 30 of treatment and almost complete repigmentation of the lesion (>75%) on day 80 of treatment. The patient tolerated the treatment well; she did not report any complaints.
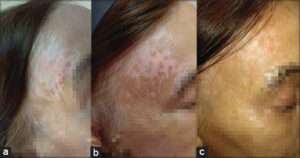 |
Figure 1: (a-c) Treatment progress of segmental vitiligo with combination of calcipotriol 0.005% and betamethasone dipropionate 0.05% in an ointment. |
Vitiligo can be divided into two types, based on location: non-segmental vitiligo (NSV), which occurs in about 90% of patients, and segmental vitiligo (SV), which occurs in about 10% of patients. NSV is typified by lesions on both sides of the body, while SV is limited to one side and usually does not cross the body’s midline [3]. Based on observations from some rare cases in 2006, a third type of vitiligo – mixed vitiligo (MV) – was proposed by Mulekar et al. MV would be the association of SV to NSV, suggesting a continuum between the previously opposed subsets. Still, MV is not yet part of the standard classification and requires more in-depth research [3].
As mentioned earlier, vitiligo is a disease with a significant genetic background and complex pathogenesis. In one publication, the frequency of vitiligo was 7% among Caucasian probands’ first-degree relatives and 6.1% for Indo-Pakistani probands. Compared to the average estimated frequencies for those individual populations (0.38% for Caucasian and 0.46% for Indo-Pakistani), the family risk was estimated to be 18-fold and 13-fold higher for each group, respectively. Statistical significance was obtained in both cases (P < 0.001) [4].
Thanks to the Genome-Wide Association Study (GWAS), more than 50 loci associated with vitiligo risk have been identified. One includes the PTPN22 gene, which encodes a protein called tyrosine phosphatase that is involved in T-cell signalling. The X-chromosome gene FOXP3 has also been found to be a risk factor for vitiligo in several ethnic groups. Other genes likely involved in the pathogenesis of vitiligo include NLRP1, XBP1, PDGFRA, IKZF4, FOXP3, and DDR1 [5].
The literature has several hypotheses about the mechanism of vitiligo, including melanocytorrhagia, oxidative stress, autoimmune, and neural mechanisms. While many of these mechanisms may be involved according to convergence theory, the autoimmune hypothesis is currently leading the way. CD8+ T cells and interferon-γ (IFN-γ) seem to play a central role in this multi-stage process [6].
Diagnosis of vitiligo should be based on clinical examination showing depigmented pearly-white patches with distinct flat dark borders on the hands, forearms, feet, and face, favouring a periocular or perioral distribution. Diagnosis usually does not require laboratory tests. The absence of melanocytes in the lesion can be assessed with confocal microscopy. In addition, a Wood’s lamp can be used to detect areas of depigmentation that may not be visible to the naked eye in the form of blue fluorescence with sharp demarcations. Dermoscopy may be useful in assessing disease activity and in differential diagnosis. Differential diagnosis should include other entities characterized by depigmentation-hypopigmentation, such as nevus depigmentosus, lichen planus, idiopathic guttate hypomelanosis, pityriasis versicolor, progressive macular hypomelanosis, drug-induced leukoderma, and hypopigmented mycosis fungoides. It is crucial to distinguish vitiligo from melanoma-related vitiligo [6].
Topical corticosteroids continue to be the first line of treatment [3]. The drug that was used in our case is a combination of calcipotriol 0.005% and betamethasone dipropionate 0.05% in ointment form. Calcipotriol is a synthetic derivative of vitamin D3 (1,25[OH]2D3) mainly used in the topical treatment of psoriasis. However, topical calcipotriol has recently been used to treat vitiligo in monotherapy or in combination therapy with steroids. The exact role of calcipotriol in melanogenesis is not yet known. Some researchers have suggested that 1,25(OH)2D3 is involved in the regulation of melanin synthesis, acting on the specific activation of T lymphocytes, affecting melanocyte maturation and differentiation, and regulating melanogenesis. One randomized trial showed that combination therapy seems to give a much faster onset of repigmentation along with better stability of the achieved pigmentation and fewer side effects [7]. Results of topical immunomodulators like tacrolimus and pimecrolimus are comparable to those of corticosteroids. Symptoms of repigmentation are also observed after phototherapy, and narrowband UVB phototherapy is the method of choice [3].
In summary, Vitiligo has been treated for many years, but only recently, when we have learned more about its pathomechanisms, it can be treated more effectively and safely.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Rahimi BA, Farooqi K, Fazli N. Clinical patterns and associated comorbidities of vitiligo in Kandahar, Afghanistan. A case-control study. Our Dermatol Online. 2020;11:6-12.
2. Ouédraogo NA, Ouédraogo MS, Tapsoba GP, TraoréF, Tamalgo PF, Ilboudo L, et al. Vitiligo and quality of life:On fi fty cases in Ouagadougou, Burkina Faso. Our Dermatol Online. 2022;13:268-72.
3. Speeckaert R, van Geel N. Vitiligo:An Update on pathophysiology and treatment options. Am J Clin Dermatol. 2017;18:733-44.
4. Alkhateeb A, Fain PR, Thody A, Bennett DC, Spritz RA. Epidemiology of vitiligo and associated autoimmune diseases in Caucasian probands and their families. Pigment Cell Res. 2003;16:208–14.
5. Marchioro HZ, Silva de Castro CC, Fava VM, Sakiyama PH, Dellatorre G, Miot HA. Update on the pathogenesis of vitiligo. An Bras Dermatol. 2022;97:478-90.
6. Bergqvist C, Ezzedine K. Vitiligo:a review. Dermatology. 2020;236:571-92.
7. Kumaran MS, Kaur I, Kumar B. Effect of topical calcipotriol, betamethasone dipropionate and their combination in the treatment of localized vitiligo. J Eur Acad Dermatol Venereol. 2006;20:269-73.
Notes
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-0719-1754http://orcid.org/0000-0001-6817-606Xhttp://orcid.org/0000-0002-3938-5679 http://orcid.org/0000-0003-0719-1754http://orcid.org/0000-0001-6817-606Xhttp://orcid.org/0000-0002-3938-5679 |

Comments are closed.