Trichoscopy of connectivitises: Discoid lupus erythematosus or dermatomyositis?
Fatima Zahra Hashas 1, Sara Elloudi1, Sara El Ammari1, Hanane Baybay1, Zakia Douhi1, Moncef Maiouak2, Fatima Zahra Mernissi1
1, Sara Elloudi1, Sara El Ammari1, Hanane Baybay1, Zakia Douhi1, Moncef Maiouak2, Fatima Zahra Mernissi1
1Department of Dermatology, University Hospital center Hassan II, Fez, Morocco, 2Department of Epidemiology and Public health, Faculty of Medicine, University Sidi Mohammed Ben Abdellah, Fez, Morocco
Citation tools:


Copyright information
© Our Dermatology Online 2023. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Background: Discoid lupus erythematosus (DLE) and Sdermatomyositis (DM) are two connectivitises with frequent scalp involvement and similar clinical features.
Objective: The objective of this study was to evaluate and compare the trichoscopic findings in patients with DM and DLE and to determine the distinctive feature of each pathology that may help in the differential diagnosis.
Materials and Methods: We performed an analytical, comparative primary study of trichoscopic images belonging to 32 patients (18 cases of lupus and 14 of dermatomyositis) with a total of seventy lesions over a period of two years.
Results: Eighteen cases of discoid lupus and fourteen cases of dermatomyositis were included. Trichoscopic founding revealed that abnormalities of follicular openings, pigment disorders, white structures, and downy hair were more frequent in lupus, and vascular patterns and dystrophic and circular hair were more prominent in dermatomyositis. The analytical study revealed that the absence or reduced number of follicular openings (p = 0.024), the presence of sliding sheaths (p = 0.048) were significant signs in favor of lupus; and the presence of perifollicular erythema (p = 0.0001), linear fine vessels and telangiectasia (p = 0.031), and pseudo-lake structures (p = 0.002) were associated with dermatomyositis.
Conclusion: Trichoscopic examination is a valuable tool for the diagnosis of connectivitis.
Key words: Trichoscopy, Scalp, Dermatomyositis, Lupus
INTRODUCTION
Discoid lupus erythematosus (DLE) and dermatomyositis (DM) are two connectivitises with frequent involvement of the scalp. Distinguishing the two conditions in a given location may be difficult as they share similar clinical features. Trichoscopic features may provide diagnostic support and differentiate between the two conditions. However, no direct comparison of these features has been made in patients with connective tissue disease. The purpose of this study was to evaluate and compare trichoscopic findings in patients with DM and DLE and to identify the characteristics of each pathology that could be helpful in differential diagnosis.
MATERIALS AND METHODS
We performed an analytical, comparative study of trichoscopic images belonging to 32 patients (18 cases of lupus and 14 of dermatomyositis) with a total of seventy lesions at the dermatology department of University Hospital Center HASSAN II in Fez, Morocco, over a period of two years from 2020 to 2022.
The inclusion criteria were the presence of clinical scalp involvement in patients with a diagnosis of DM and DLE.
The exclusion criteria were: overlapping connectivitises, the presence of other pathologies affecting the scalp, and the use of drugs affecting the hair growth/color cycle.
All patients were examined with the DermLite DL4 digital dermoscope with minimal pressure, and photographs were taken in several scalp locations.
The trichoscopic evaluation focused on several aspects: follicular openings, follicular stalk, perifollicular surface, interfollicular space, white structures, vascularization.
The data was entered in an Excel sheet, analyzed with SPSS, version 26, and compared with the chi-squared test.
RESULTS
There were eighteen cases of discoid lupus (1 male, 17 females), with a male-to-female ratio of 0.05 and a mean age of forty years. The clinical patterns were as follows: single alopecic patch (22%) and multiple alopecic patches (78%). The average duration of evolution was seven years.
There were fourteen cases of dermatomyositis (3 males, 11 females), with a male-to-female ratio of 0.27 and an average age of fifty years. The clinical patterns were as follows: diffuse alopecia (50%), alopecic patches (14%), and no alopecia (36%). The average duration of evolution was six years.
Table 1 summarizes the different trichoscopic characteristics of the two pathologies.
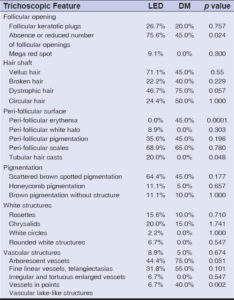 |
Table 1: Comparison of trichoscopic features in the patients with discoid lupus and dermatomyositis. |
Abnormalities of the follicular openings, pigment disorders, white structures, and downy hair were more frequent in lupus (Fig. 1), while vascular patterns, dystrophic, and circular hair were more prominent in dermatomyositis (Fig. 2).
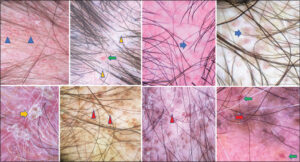 |
Figure 1: Scalp discoid lupus erythematosus. Trichoscopic features: scattered brown spotted pigmentation (black arrow); microhemorrhage (yellow arrow); scales (blue circle); arborescent vessels (triangle jaune); chrysalids (green triangle); pinkish-white background (red asterisk); follicular keratotic plugs (black triangle); tubular hair casts (black triangle). |
 |
Figure 2: Scalp dermatomyositis. Trichoscopic features: enlarged, irregular, and tortuous capillaries (blue triangle); vascular, lake-like structures (green arrows); chrysalids (yellow triangle); perifollicular erythema (blue arrows); scales (yellow arrows); peri-follicular pigmentation (red triangle); interfollicular pigmentation (red arrows). |
The analytical study revealed that the absence or reduced number of follicular openings (p = 0.024) and the presence of sliding sheaths (p = 0.048) were significant signs in favor of lupus; and the presence of perifollicular erythema (p = 0.0001), linear fine vessels and telangiectasia (p = 0.031), and pseudo-lake structures (p = 0.002) were associated with dermatomyositis.
DISCUSSION
Scalp involvement is common in connectivitis and negatively impacts the patient’s quality of life [1,2], In this location, clinical signs may overlap and present a diagnostic challenge. Trichoscopy may be of great help and provide distinctive diagnostic clues. However, only several studies have presented this information [3–6]. A direct comparison of the trichoscopic findings in DM and SLE is lacking.
In DM, scalp lesions may present as erythema owing to photosensitivity or atrophic and erythematous-scaly lesions frequently accompanied by pruritus. Scalp poikiloderma and non-scarring alopecia may also occur [7–9]. Trichoscopy seems to be a useful non-invasive tool in diagnosing this condition. The first study on trichoscopy features of scalp dermatomyositis was published by Julio et al. in 2017 [5], who described scalp involvement in thirty-one patients with DM. Twenty-eight patients were evaluated by trichoscopy. The most consistent findings were the presence of enlarged capillaries, found in 20 (71.4%) cases, followed by peripilar casts (57.1%) and tufting and interfollicular scales in 14 (50%) cases.
Żychowska et al. recently reported trichoscopic findings in 15 DM patients. The most common findings were as follows: linear branched vessels (80.0%), linear vessels (60.0%), linear curved vessels (53.3%), perifollicular pigmentation (40.0%), perifollicular erythema (33.3%), scaling (20.0%), white (20.0%) or yellow (20%) interfollicular scales, and white (20.0%) or pinkish (13.3%) structureless areas [7].
In DLE, scalp involvement is frequent and inaugural in more than half of cases and may remain isolated in 10% of cases [10]. Females are primarily affected and these tend to be young (mean age: 30 years). The scalp is affected in the form of single or multiple alopecic plaques, well limited, inflammatory, and scaly with follicular hyperkeratosis at the beginning, then secondarily atrophic and dyschromic, leaving definitive scarring alopecia after healing [11].
The dermatoscopic appearance reported in DLE varies according to the stage of evolution. A recent systematic review of the literature summarized and analyzed the dermoscopic features of DLE lesions in various anatomical locations. In scalp DLE, the most common findings were as follows: white structureless areas (62%), arborizing vessels (57.8%), white scales (54.2%), follicular keratotic plugs (47%), absent follicular openings (45.8%), perifollicular scaling (43.9%), pinkish-white background (40.4%), speckled brown pigmentation (38%), and fibrotic white dots (33.7%) [12].
The present study provided new insights into the trichoscopic values of patients with DM and DLE. To our knowledge, we are the first to compare trichoscopic features among these two conditions. We identified distinctive findings that may help in differentiating the two entities.
The pseudo-lake vascular structures (defined as ectatic vascular structures filled with red-blood cells) reported in a study by Julio [5] were associated with dermatomyositis in our study [2]. The absence or reduced number of follicular openings were specific signs in discoid lupus.
CONCLUSION
Scalp involvement is prevalent in discoid lupus erythematosus (DLE) and dermatomyositis (DM). Our study allowed us to determine the specific trichoscopic features of each pathology that could help in the differential diagnosis.
Statement of Human and Animal Rights
All the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the 2008 revision of the Declaration of Helsinki of 1975.
Statement of Informed Consent
Informed consent for participation in this study was obtained from all patients.
REFERENCES
1. Cassano N, Amerio P, D’Ovidio R, Vena GA. Hair disorders associated with autoimmune connective tissue diseases. G Ital Dermatol Venereol. 2014;149:555-65.
2. Ferraz LB, Almeida FA, Vasconcellos MR, Faccina AS, Ciconelli RM, Ferraz MB. The impact of lupus erythematosus cutaneous on the quality of life:The Brazilian-Portuguese version of DLQI. Qual Life Res. 2006;15:565-70.
3. Suchonwanit P, Udompanich S, Thadanipon K, Chanprapaph K. Trichoscopic signs in systemic lupus erythematosus:A comparative study with 109 patients and 305 healthy controls. J Eur Acad Dermatol Venereol. 2019;33:774-80.
4. Kwiatkowska M, Rakowska A, Walecka I, Rudnicka L. The diagnostic value of trichoscopy in systemic sclerosis. J Dermatol Case Rep. 2016;10:21–5.
5. Jasso-Olivares JC, Tosti A, Miteva M, Domínguez-Cherit J, Díaz-González JM. Clinical and dermoscopic features of the scalp in 31 patients with dermatomyositis. Skin Appendage Disord. 2017;3:119-24.
6. Chanprapaph K, Limtong P, Ngamjanyaporn P, Suchonwanit P. Trichoscopic Signs in dermatomyositis, systemic lupus erythematosus, and systemic sclerosis:A comparative study of 150 patients. Dermatology. 2022;238:677-87.
7. Żychowska M, Reich A. Dermoscopy and trichoscopy in dermatomyositis:A cross-sectional study. J Clin Med. 2022;11:375.
8. Kasteler JS, Callen JP. Scalp involvement in dermatomyositis:Often overlooked or misdiagnosed. JAMA. 1994;272:1939-41.
9. Tilstra JS, Prevost N, Khera P. Scalp dermatomyositis revisited. Arch Dermatol. 2009;145:1062-3.
10. Francès C. Manifestations cutanées des lupus érythémateux. EMC-Dermatologie. 2015;10:1-14.
11. Pruvost C, Reygagne P. Alopécies cicatricielles. EMC – Dermatologie. Paris:Elsevier Masson SAS. 2009;98-810-B-20.
12. Żychowska M. Dermoscopy of discoid lupus erythematosus:A systematic review of the literature. Int J Dermatol. 2021;60:818-28.
Notes
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0002-5360-337Xhttp://orcid.org/0000-0002-5942-441Xhttp://orcid.org/0009-0001-8083-1730http://orcid.org/0000-0003-3455-3810 http://orcid.org/0000-0002-5360-337Xhttp://orcid.org/0000-0002-5942-441Xhttp://orcid.org/0009-0001-8083-1730http://orcid.org/0000-0003-3455-3810 |

Comments are closed.