What does a clown’s nose reveal?
Sokaina Chhiti , Hanane Baybay, Fatima Zahra Hashas, Zakia Douhi, Meryem Soughi, Sara Elloudi, Fatima Zahra Mernissi
, Hanane Baybay, Fatima Zahra Hashas, Zakia Douhi, Meryem Soughi, Sara Elloudi, Fatima Zahra Mernissi
Department of Dermatology, University Hospital Hassan II, Fez, Morocco
Citation tools:


Copyright information
© Our Dermatology Online 2023. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
Numerous diseases may cause a reddish swelling on the tip of the nose yet do not produce a lump. A clown’s nose (CN) is a condition characterized by a rapidly growing mass resembling a clown’s false red nose, which invariably suggests the presence of usually secondary and rarely primary malignancy. This localization requires careful excision with impeccable preoperative, intraoperative, and postoperative scar planning in order to obtain an acceptable aesthetic result. Herein, we report the case of a patient with a clown’s nose appearance revealing a giant primary cutaneous squamous cell carcinoma.
A 65-year-old patient with no pathological history consulted for an enlargement of the nose present for a year. An examination revealed a red, fixed mass of 4 cm, surmounted by scales at the level of the nose in endonasal extension (Fig. 1a). On dermoscopy, an erythematous background, tree-trunk vessels, scales, and keratin were present (Fig. 1b). An initial skin biopsy revealed granulomatous dermatitis with reactive lymphocytic infiltrate. In view of the endonasal component and the clinical appearance, a second biopsy was performed, suggesting nasal T-cell lymphoma, granulomatous rosacea, and mucocutaneous leishmaniasis, the results of which were in favor of squamous cell carcinoma (SCC). An extension assessment comprising ultrasound of the lymph nodes and cerebral, thoracic, and abdominal scans were unremarkable, and the patient benefited from an enlarged excision with healthy margins associated with scar support based on local care (Fig. 2), antibiotic therapy orally, and healing cream until healing. Then, adjuvant radiotherapy sessions were performed to allow the reconstruction procedure, yet the patient refused the procedure.
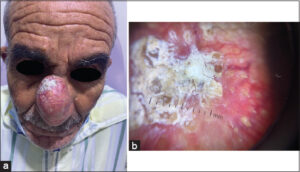 |
Figure 1: (a) Giant tumor on the nose topped with scales (b) Dermoscopy showing fundus erythematous, keratin, tree-trunk vessels. |
 |
Figure 2: Clinical aspect after surgical excision. |
A clown’s nose (CN) is usually due to pulmonary, metastatic breast cancer or other diseases, rarely due to primary neoplasms such as squamous cell and basal cell carcinoma [1]. Several articles describe what may be defined as a CN [2,3]. Generally, the CN is due to a cutaneous metastasis of a known lung or breast cancer, of which only a histological examination makes it possible to distinguish these secondary malignancies from primary cutaneous squamous cell or basal cell carcinomas.
In only one article, the cause was a basal cell carcinoma [4] and, in another, a squamous cell carcinoma [5]. Our patient was the second case in which an SCC was involved. SCC usually affects elderly patients with a personal history of excessive sun exposure and fair skin types, as was the case of our patient.
Recently, Zhao et al. divided the CN into three groups: metastatic solid tumors, genetic diseases, and diseases involving the nasal tip. The clown’s nose appearance is an indirect sign of the development of neoplasia [1].
Tumor-related tissue reactions leading to the formation of epithelioid cell granulomas have been known for almost seventy years. Such reactions may occur in the lymph nodes draining an area harboring a malignant tumor, in the tumor itself, and even in non-regional tissues [6]. They occur in 4.4% of carcinomas. Most likely, they are due to antigenic factors derived from tumor cells, causing an immunological hypersensitivity reaction leading to the formation of epithelioid cell granulomas [7]. It may be a good prognostic marker of the antitumor response against metastatic extension. In our case, the first biopsy showed a granulomatous reaction with a negative extension assessment.
Finally, a multidisciplinary approach involving dermatologists, maxillofacial/plastic surgeons, oncologists, and radiotherapists is also recommended for minor cutaneous malignancies in order to obtain optimal and aesthetic results.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Zhao B, Chen L, Liao J, Xie Z, Lei X, Shen Z. Update of clown nose-like lesion, a underrecognized manifestation of metastatic malignancies and genetic cancer Predisposition Syndromes. Front Med. 2021;8:673336.
2. Chun SM, Kim YC, Lee JB, Kim SJ, Lee SC, Won YH, et al. Nasal tip cutaneous metastases secondary to lung carcinoma:Three case reports and a review of the literature. Acta Derm Venereol. 2013;93:569-72.
3. Gomez-Zubiaur A, Trasobares-Marugán L, Aboín-González S, Medina-Expósito I, Villalobos-León ML. Solitary cutaneous metastasis of renal clear cell carcinoma on nasal tip. Melanoma Res. 2016;26:E108-9.
4. Aneiros-Fernandez J, Arias-Santiago S, Garcia-Lopez C, O’Valle F. Disfiguring basal cell carcinoma of the nose (“clown nose“). Ear Nose Throat J. 212;91:E26-7.
5. Colletti G, Allevi F, Moneghini L, Palvarini M. Clown nose:A case of disfiguring nodular squamous cell carcinoma of the face. BMJ Case Rep. 2014;bcr 2013200471.
6. Pavic M, Debourdeau P, Vacelet V, Rousset H. [Sarcoidosis and sarcoid reactions in cancer]. Rev Med Interne. 2008;29:39-45.
7. Brincker H. Sarcoid reactions in malignant tumours. Cancer Treat Rev. 1986;13:147-56.
Notes
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0009-0000-6899-8637http://orcid.org/0000-0003-3455-3810http://orcid.org/0000-0002-5360-337Xhttp://orcid.org/0000-0002-5942-441X http://orcid.org/0009-0000-6899-8637http://orcid.org/0000-0003-3455-3810http://orcid.org/0000-0002-5360-337Xhttp://orcid.org/0000-0002-5942-441X |

Comments are closed.