A strange umbilical rash in a newly diagnosed HIV-positive male: A new clinical description of Trichosporon spp. dermatosis
Ryme Dassouli 1, Zakia Douhi1, Kenza Tahiri Joutei1, Hanane BayBay1, Sara Elloudi1, Khaoula Abdellaoui2, Laila Tahiri2, Hinde El Fatemi2, Fatima Zahra Mernissi1
1, Zakia Douhi1, Kenza Tahiri Joutei1, Hanane BayBay1, Sara Elloudi1, Khaoula Abdellaoui2, Laila Tahiri2, Hinde El Fatemi2, Fatima Zahra Mernissi1
1Department of Dermatology, University Hospital Hassan II, Fes, Morocco, 2Department of Anatomopathology, University Hospital Hassan II, Fes, Morocco
Citation tools:


Copyright information
© Our Dermatology Online 2023. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
Trichosporon is a basidiomycete yeast of tropical origin that is also opportunistic in the immunocompromised. It is characterized by irregular nodules attached to the hair known as white piedra. Trichosporon spp. have been reported as the second most common agent of disseminated, potentially fatal fungemia [1]. Nevertheless, no pure cutaneous manifestation has been reported. Herein, we report a single case of Trichosporon spp. causing an umbilical papulonodular rash in a newly diagnosed HIV-positive individual.
A 25-year-old patient, with a history of homosexuality and unprotected sexual intercourse, presented with a one-week-old, asymptomatic, reddish rash associated with umbilicated, papular lesions of the trunk and lower back, which were pruritic and concomitant in appearance. A dermatological examination revealed scattered, copper-red papules on the face, trunk, and limbs, palmo-plantar, papular lesions surrounded by a thin, circular, whitish collar, with large papules and nodules with an umbilicated center, pruritic and eroded, located in the sacral region and pre-pectoral area (Figs. 1a and 1b). Dermoscopy revealed a star-like appearance with erythema in the center, whitish lines in a radial arrangement surrounded by a crown of vessels in points (Fig. 2). A mucosal examination revealed a syphilitic chancre on the glans. The lymph nodes were free. The rest of the examination was unremarkable. HIV and syphilitic serology were positive, with a VDRL titer of 1/64. The lumbar puncture was sterile. A biopsy of the umbilical lesions was performed, which revealed sheets of inflammatory cells consisting essentially of macrophages forming nodules around the vascular structures of the superficial and deep dermis. Microscopic yeasts were present in the macrophagic cytoplasm. A mycological study on the collected tissue revealed the presence of Trichosporon spp. The diagnosis of an opportunistic infection with Trichosporon spp. in an HIV-positive and syphilitic individual in the second bloom phase was accepted. The patient was treated with late penicillin for syphilis, and antiretroviral treatment was recommended after a normal pre-treatment workup. Three weeks later, the syphilis disappeared and the nodular lesions subsided. Dermoscopy of the lesions revealed the disappearance of the star-like appearance with the presence of vessels in points and the attenuation of the erythema.
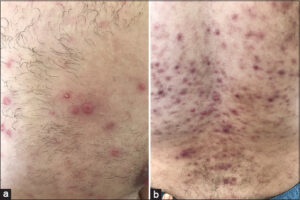 |
Figure 1: (a) and (b) Umbilical, papulonodular lesions of the trunk. |
 |
Figure 2: Dermoscopy showing a star-like appearance with erythema in the center, whitish lines in a radial arrangement that were surrounded by a crown of vessels in points. |
Trichosporon are natural soil inhabitants as well as components of the human skin and nail flora, which, in tropical climates, may cause benign, superficial hair lesions (piedra blancs), characterized by the presence of irregular nodules on the affected hair [2]. These nodules are loosely attached to the hair shaft, have a soft texture, and may be white or light brown [3].
David et al. reported a case of lichenoid lesions of the trunk in an HIV-positive patient, in whom histological and mycological studies revealed the coexistence of Trichosporon and Histoplasma capsulatum during systemic fungemia [4].
In our case, the association of a syphilitic chancre and asymptomatic coppery papular lesions of the body with nail-like palmar lesions surrounded by Biett’s collarette represented the typical aspect of syphilis in coexistence with primary syphilis, frequently encountered in seropositive individuals. HIV serology was, then, requested together with syphilitic serology to confirm the diagnosis of syphilis, which returned positive. Moreover, the papulo-nodular lesions of the trunk and lower back had a different appearance, with an umbilical and pruritic character. Two hypotheses were evoked: syphilis with an atypical clinical presentation in a seropositive individual or a cutaneous fungal co-infection such as histoplasmosis, cryptococcosis, or penicilliosis. Histology revealed yeasts in the papillary and reticular dermis surrounded by inflammatory cells, and further mycological analysis confirmed the presence of Trichosporon spp.
The clinical form of this fungus in our patient indicated a good therapeutic response to Penicillin G. However, previous studies have demonstrated positive antifungal activity with azoles and amphotericin B treatment for Trichosporon infection [5]. Other forms of treatment, such as the resection of the infected tissue, are associated with greater improvement [5,6].
Herein, we have reported an original case of opportunistic fungal dermatosis in an HIV-positive individual with a good therapeutic response to penicillin. Indeed, a Trichosporon infection should not be excluded in front of umbilical eruptions in an immunocompromised patient. Although not reported in the literature, the efficacy of penicillin against this mycosis remains to be demonstrated.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Rajput PS, Das AK, Paudel U, Parajuli S. Mucocutaneous disorders in HIV/AIDS at a tertiary care hospital in Nepal:An observational study. Our Dermatol Online. 2021;12:101-5.
2. Maddy AJ, Sanchez N, Shukla BS, Maderal AD. Dermatological manifestations of fungal infection in patients with febrile neutropaenia:A review of the literature. Mycoses. 2019;62:826-34.
3. Hajjar J, Restrepo A, Javeri H, Wiederhold NP, Papanastassiou AM, Patterson TF. Multiple Brain Abscesses Caused by Trichosporon inkin in a Patient with X-Linked Chronic Granulomatous Disease (CGD) Successfully Treated with Antifungal Therapy. J Clin Immunol. 2017;37:519-23.
4. Barro/TraoréF, Sanwidi M, Dao F, Korsaga/SoméN, Niamba P, TraoréA, et al. [Disseminated African histoplasmosis in an immunocompetent child in Burkina Faso:One case]. Our Dermatol Online. 2013;4:361-8.
5. Mancy A. Chronic dermatophytosis:A clinical, epidemiological, mycological study. Our Dermatol Online. 2022;13:36-40.
6. Ouédraogo NA, Kouassi AA, Ouédraogo MS, Somda KS, Tapsoba GP, Ouangre/Ouédraogo A, et al. [Peritoneal and pericardial involvements of multifocal African histoplasmosis on sever undernutrition]. Our Dermatol Online. 2021;12(Supp. 2):16-20.
Notes
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-4330-4429http://orcid.org/0000-0003-3455-3810http://orcid.org/0000-0002-5942-441Xhttp://orcid.org/0000-0002-2848-7549 http://orcid.org/0000-0003-4330-4429http://orcid.org/0000-0003-3455-3810http://orcid.org/0000-0002-5942-441Xhttp://orcid.org/0000-0002-2848-7549 |

Comments are closed.