Clinical, dermoscopic and histopathological description of hyperkeratotic porokeratosis of Mibelli
Chaymae Jroundi 1, Hanane Baybay1, Jihad Kassel1, Samia Mrabat1, Zakia Douhi1, Sara Elloudi1, Fatima Zahra Mernissi1, Mouna Rimani2
1, Hanane Baybay1, Jihad Kassel1, Samia Mrabat1, Zakia Douhi1, Sara Elloudi1, Fatima Zahra Mernissi1, Mouna Rimani2
1Department of Dermatology, University Hospital Hassan II, Fes, Morocco, 2Hassan Center of Pathology, Rabat, Morocco
Citation tools:


Copyright information
© Our Dermatology Online 2023. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
Porokeratosis of Mibelli is a clinical form of porokeratosis among an original set of dermatoses characterized by disorders of epidermal differentiation and keratinization. It represents one third of all cases of porokeratosis. Its etiology is not well established. It occurs most often in childhood or adolescence and predominantly in males. It is clinically characterized by one or more annular plaques with raised borders, atrophic centers, and a centrifugal evolution located on the extremities [1]. It has, recently, been reported that some cases of porokeratosis of Mibelli show a low frequency of hyperkeratotic lesions, which some authors have called the hyperkeratotic variant of porokeratosis Mibelli. Diagnostic confirmation is achieved through a histopathological examination with the finding of the cornoid lamella and hypogranulosis [2]. The hyperkeratotic variant is characterized by more severe hyperkeratosis with abundant coronal lamellae on histology. The usefulness of dermoscopy lies in the fact that it orientates the diagnosis by showing classically white, central areas without structures, dots and reddish-brown globules, and a peripheral border with a double margin translating the coronoid lamellae. Therapeutic management is based on keratolytic agents [2,3]. Herein, we present a clinical and dermoscopic description of the hyperkeratotic variant of porokeratosis of Mibelli.
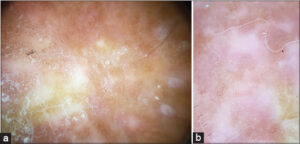
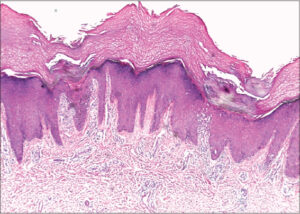
A nineteen-year-old patient with a history of peripheral spondyloarthritis presented with slightly pruritic lesions on the back of the hand persistent for five years, treated as psoriasis with topical steroids with no improvement. A clinical examination revealed multiple, verrucous, slightly erythematous, and hyperkeratotic papules located on the back of the left hand (Fig. 1). Dermoscopy without immersion showed the predominance of whitish, verrucous areas without structures, white scales, after immersion: brown spots and globules and erythema (Fig. 2). A skin biopsy was performed showing a large predominance of coronoid lamellae consisting of parakeratotic cells in a “stack of plates” resting on a sudden depression of the epidermis without a granular layer at this level and a lichenoid reaction suggesting porokeratosis of Mibelli (Fig. 3). The case of our patient differed from the classical form characterized by a rather verrucous and hyperkeratotic aspect of the lesions. This observation is, therefore, closer to the hyperkeratotic form, which is rarer. A dermoscopic description of this entity has, to the best of our knowledge, not yet been reported.

Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Jha AK, Sonthalia S, Lallas A. Dermoscopy of porokeratosis of Mibelli. Indian Dermatol Online J. 2017;8:304-5.
2. Ferreira FR, Santos LD, Tagliarini FA, Lira ML. Porokeratosis of Mibelli–Literature review and a case report. An Bras Dermatol. 2013;88(6 Suppl 1):179-82.
3. Mrabat S, Baybay H, Oujdi S, Douhi Z, Elloudi S, Mernissi FZ. Porokeratosis:A diagnosis made easy by the dermoscope!Our Dermatol Online. 2020;11:e141.1.
Notes
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-3455-3810http://orcid.org/0000-0002-5942-441X http://orcid.org/0000-0003-3455-3810http://orcid.org/0000-0002-5942-441X |

Comments are closed.