Artificial pearl-induced penile annular lichen planus
Ngo Binh Trinh 1, Giang Huong Tran2
1, Giang Huong Tran2
1Department of Venereology, Ho Chi Minh City Hospital of Dermato-Venereology, Vietnam, 2Department of Pathology, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
Annular lichen planus is an uncommonly reported variant of lichen planus, especially on the penis [1]. Herein, we report a case of penile annular lichen planus induced by artificial pearls.
A 42-year-old, circumcised male presented to our hospital with asymptomatic, annular lesions of the glans penis. Around one month prior to presentation, he reported a history of inserting artificial pearls inside his penis by stainless steel. He denied a history of drug intake or a personal history of hepatitis C. A physical examination revealed multiple, reddish-purple, annular plaques with central atrophy on the glans penis (Fig. 1a). Inguinal lymph nodes and other mucocutaneous lesions were absent.
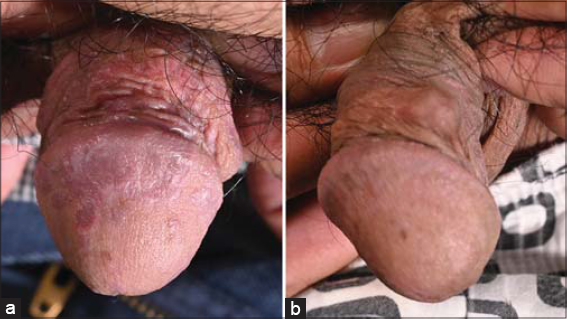 |
Figure 1: Annular lichen planus: (a) multiple, reddish-purple, annular plaques with central atrophy; (b) after two-week treatment with tacrolimus 0.1%. |
On the day of the visit, a rapid plasma reagin (RPR) test, Treponema pallidum hemagglutination (TPHA) test, and hepatitis C antibody test were all negative. Fungal microscopy of the glans penis was negative. A patch test was not performed due to its unavailability.
A histological examination revealed a lichenoid reaction pattern characterized by a combination of degeneration of the basal layer of the epidermis and a band-like lymphocytic infiltrate obscuring the dermal-epidermal junction. There was irregular, epidermal hyperplasia forming a characteristic saw-tooth appearance with wedge-shaped hypergranulosis (Fig. 2a). The basal layer of the epidermis exhibited vacuolar degeneration. The inflammatory infiltrate was chiefly lymphocytic and formed a dense band in the superficial dermis (Figs. 2b and 2c).
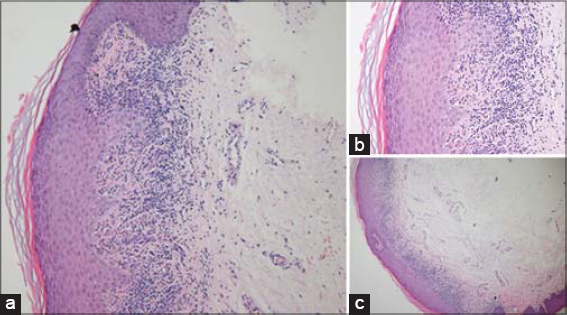 |
Figure 2: Histological findings: epidermal hyperplasia forming a characteristic saw-tooth appearance with wedge-shaped hypergranulosis (H&E, 40×); (b-c) the basal layer of the epidermis exhibiting vacuolar degeneration and the inflammatory infiltrate chiefly lymphocytic and forming a dense band in the superficial dermis (H&E, 100× and 200×). |
The diagnosis of annular lichen planus was confirmed and tacrolimus 0.1% was applied twice a day for two weeks. The lesions resolved significantly (Fig. 1b).
Annular lichen planus is one of the rarest variants of lichen planus, accounting for 3-7% of cases. The lesions present as ring-formed, violaceous plaques with or without central atrophy on the intergious sites, the penis and the scrotum [2].
The pathogenesis of lichen planus remains unknown. However, it is related to virus infection (hepatitis C), drugs (antimalarials, ACEIs, thiazide diuretic, NSAIDs, quinidine, beta-blockers, tumor necrosis factor-alpha inhibitors, gold), and contact allergens (mercury, copper, and gold) [3]. Our patient presented the annular lesions on the glans penis after one month of penile implants; therefore, it could be linked to the etiology.
The differential diagnosis of a penile annular lesion includes annular psoriasis, granuloma annulare, dermatophyte infection, and annular secondary syphilis [4]. Annular psoriasis is characterized by annular, erythematous plaques with scaling borders and central clearing, especially a positive Auspitz’s sign. Therefore, annular psoriasis was excluded due to the negativity of the Auspitz’s sign and the non-scaling borders of the lesions. Fungal microscopy and syphilis tests were negative. The diagnosis of a dermatophyte infection and annular secondary syphilis were also excluded. Granuloma annulare is histologically characterized by necrobiotic degeneration of dermal collagen surrounded by an inflammatory reaction, while the band-like lymphocytic infiltration at the dermal-epidermal junction is commonly seen in annular lichen planus.
The first-line treatment of genital lichen planus is topical corticosteroids. Alternative treatments include topical calcineurin inhibitors, topical calcipotriol, systemic corticosteroids, acitretin, isotretinoin, methotrexate, hydroxychloroquine, dapsone, cyclosporine, azathioprine, and mycophenolate mofetil [2,5].
Annular lichen planus is a rare manifestation of lichen planus, which may be misdiagnosed as other annular skin lesions.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Badri T, Kenani N, Benmously R, Debbiche A, Mokhtar I, Fenniche S. Isolated genital annular lichen planus. Acta Dermatovenerol Alp Pannonica Adriat. 2011;20:31-3.
2. Weston G, Payette M. Update on lichen planus and its clinical variants. Int J Womens Dermatol. 2015;1:140-9.
3. Farhi D, Dupin N. Pathophysiology, etiologic factors, and clinical management of oral lichen planus, part I:Facts and controversies. Clin Dermatol. 2010;28:100-8.
4. Zhao C-C, Zhang Z, Zheng S, Li J-H. Annular secondary syphilis on the penis:A case report. Int J Dermatol Venereol. 2019;2:118-9.
5. Mai S, Mansouri S, Hassam B. Annular atrophic lichen planus. BMJ Case Reps. 2019;12:e229270.
Notes
Source of Support: Nil,
Conflict of Interest: The authors have no conflict of interest to declare.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0002-3829-3115http://orcid.org/0000-0002-9480-4602 http://orcid.org/0000-0002-3829-3115http://orcid.org/0000-0002-9480-4602 |

Comments are closed.