Aggressive epithelioid hemangioendothelioma of the forearm with scalp metastasis: A case report
Asmae Abdelmouttalib 1, Soumaya Hamich2, Amine Haouzi1, Mariame Meziane1, Nadia Ismaili1, Leila Benzekri1, Karima Senouci1
1, Soumaya Hamich2, Amine Haouzi1, Mariame Meziane1, Nadia Ismaili1, Leila Benzekri1, Karima Senouci1
1Dermatology and Venereology Department, Mohamed V University in Rabat, Morocco, 2Traumatology Department, Mohamed V University in Rabat, Morocco
Corresponding author: Asmae Abdelmouttalib
Submission: 02.06.2021; Acceptance: 09.10.2021
DOI: 10.7241/ourd.20223.13
Cite this article: Abdelmouttalib A, Hamich S, Haouzi A, Meziane M, Ismaili N, Benzekri L, Senouci K. Aggressive epithelioid hemangioendothelioma of the forearm with scalp metastasis: A case report. Our Dermatol Online. 2022;13(3):296-298.
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Epithelioid hemangioendothelioma (EHE) is an extremely rare sarcoma whose target may be different organs, including soft tissue. The spectrum of the disease is highly variable between indolent and aggressive with extended metastases. Herein, we report a case of epithelioid hemangioendothelioma in the left forearm that progressed quietly for ten years before local and distant metastases appeared. Our case report aims to insist on the interest in the management of such tumors at an early stage because of the possible evolution toward metastasis, even after several years of asymptomatology.
Key words: Hemangioendothelioma; Epithelioid; Soft tissue; Vascular tumor; Metastasis
INTRODUCTION
Epithelioid hemangioendothelioma (EHE) is an extremely rare sarcoma and, as such, may pose a clinical dilemma based solely on its rarity. In addition, the spectrum of the disease is highly variable between indolent and aggressive with extended metastases [1].
Herein, we report a case of epithelioid hemangioendothelioma in the left forearm that progressed quietly for ten years before local and distant metastases appeared.
CASE REPORT
A 38-year-old female presented for dermatological consultation with multiple tumors on the scalp evolving for the previous eight months. Her medical history was insignificant except for a tumor on the left forearm, neglected by the patient, having evolved for the last ten years and having gradually increased in volume. The evolution was marked during these last months by the appearance of pain in the tumefaction of the forearm as well as motor and sensory disorders of the same upper limb. She also presented a notion of weight loss calculated at 10 kg with asthenia. A general clinical examination found a cachexic and dyspneic patient. At the scalp level, the patient presented several ulcerated nodules, painful on palpation, with raised edges and indurated bases. The largest nodule measured 4 cm in its long axis (Fig. 1). On the left forearm, there was a tumor, soft and very painful, fixed at the deep plane. A neurological examination revealed a defect in the finger spacing capacity and in the overall grip of the hand. The rest of the clinical examination was unremarkable. A deep biopsy of the tumor from the forearm performed by traumatologists revealed an epithelioid hemangioendothelioma with foci of necrosis. A scalp biopsy confirmed skin metastases of the same malignant process. The rest of the extension assessment, which included cerebral and thoraco-abdominal CT scans, showed a secondary localization in the lungs (Fig. 2). MRI of the upper left extremity revealed a tissue mass in the anterior compartment of the forearm with bone invasion (Fig. 3). Although chemotherapy was recommended, the patient’s condition deteriorated and she died the following month.
 |
Figure 1: Several ulcerated nodules with raised borders in favor of skin metastases. |
 |
Figure 2: Secondary localization in the lungs. |
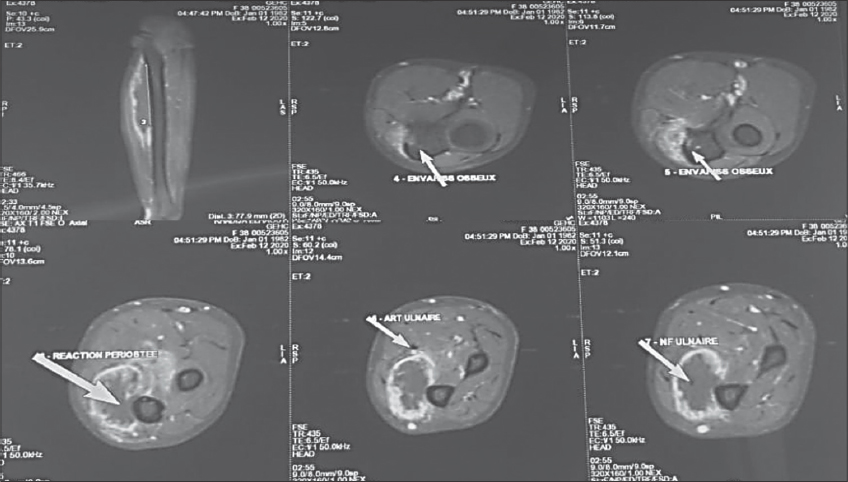 |
Figure 3: A tissue mass in the anterior compartment of the forearm with bone invasion: a periosteal reaction with a cortical rupture at the ulna and a compassion of the ulnar and median nerves (white arrows). |
DISCUSSION
EHE develops from vascular endothelial or pre-endothelial cells and any site in the body (bones, soft tissue, and other organs: lungs, liver, spleen, brain, breasts, heart) may be a target for the disease [2,3]. Epithelioid hemangioendothelioma (EHEM) of soft tissue is rare and is observed in middle-aged adults, rarely during childhood, and in both males and females [4].
The spectrum of the disease varies greatly between indolent and aggressive with widespread metastases [1]. It is characterized by clinical latency with a consultation time of up to ten years or more in one third of patients [5]. Occasionally, a patient may present with systemic manifestations such as weight loss and anemia, as in our patient [2,6]. Patients who are symptomatic or have a metastasis on presentation have a worse prognosis [7]. Histologically, it is an angiocentric vascular tumor consisting of epithelial endothelial cells in a fibro-myxoid stroma [5]. Some histological signs are correlated with a more aggressive tumor evolution and are found in 30% of cases of HEE: the presence of atypia, foci of necrosis, mitosis > 1mitosis per 10 fields under high magnification (40×) and foci of spindle-shaped cells [4,5,7]. In our case, large foci of necrosis were present. The treatment varies depending on the grade of malignancy. The treatment of low-grade forms of malignancy is essentially based on marginal resection with strict monitoring. In multicentric forms, adjuvant radiotherapy is indicated and seems to be effective. For high-grade forms of malignancy, the treatment consists of more radical surgery, while for aggressive multifocal forms, polychemotherapy has been used yet without efficacy [7]. New targeted agents such as pazopanib and afatinib have demonstrated anecdotal efficacy [1].
CONCLUSION
Our case report aims to insist on the importance of initially evaluating the aggressive nature of the disease, which will then dictate how urgently the patient needs to be treated.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Rosenberg A, Agulnik M. Epithelioid hemangioendothelioma:Update on diagnosis and treatment. Curr Treat Options Oncol. 2018;4:15-19.
2. Sardaro A, Bardoscia L, Petruzzelli MF, Portaluri M. Epithelioid hemangioendothelioma:An overview and update on a rare vascular tumor. Oncol Rev. 2014;2:258-9.
3. Sporn TA. Epithelioid hemangioendothelioma of the pleura:An aggressive vascular malignancy and clinical mimic of malignant mesothelioma. Histopathology. 2002;41:173-7.
4. Deyrup AT, Tighiouart M, Montag AG, Weiss SW. Epithelioid hemangioendothelioma of soft tissue:A proposal for risk stratification based on 49 cases. Am J Surg Pathol. 2008;32:924-7.
5. Fletcher CDM. Lyon:IARC Press;2002. Tumors of soft tissue and bone Pathology and Genetics.
6. Bagan P, Hassan M, Le Pimpec Barthes F, Peyrard S, Souilamas R, Danel C, et al. Prognostic factors and surgical indications of pulmonary epithelioid hemangioendothelioma:A review of the literature. Ann Thorac Surg. 2006;82:2010-3.
7. Hannachi Sassi S, Mansouri D, Abbes I, Dhouib R, Driss M, Mrad K, Ben Ayed F, Ben Romdhane K. [Soft tissue epithelioid hemangioendothelioma:A case report]. Rev Chir Orthop Reparatrice Appar Mot. 2005;91:671-5.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.