Dermoscopy of pilomatricoma: A case report with a review of the literature
Radia Chakiri 1,2, Youssef Bouhajeb3
1,2, Youssef Bouhajeb3
1Department of Dermatology, University Hospital Agadir, Morocco, 2Faculty of Medicine and Pharmacy Agadir, University Ibn Zohr, Agadir, Morocco, 3Center of Pathology Ibn Rochd, Agadir, Morocco
Corresponding author: Radia Chakiri, MD
How to cite this article: Chakiri R, Bouhajeb Y. Dermoscopy of pilomatricoma: A case report with a review of the literature. Our Dermatol Online. 2022;13(1):82-85.
Submission: 08.04.2021; Acceptance: 05.08.2021
DOI: 10.7241/ourd.20221.20
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Pilomatricoma is a benign tumor originating from hair follicle matrix cells and characterized by the presence of cutaneous and subcutaneous nodules up to 3.0 cm in diameter, usually on the head, neck, and upper extremities, rarely on the trunk and lower extremities. An eleven-year-old female with a painless, erythematous-purplish tumor of the back. A dermoscopic examination revealed irregular linear vessels, white structures, and structureless grayish-blue areas. Histological examination after excision confirmed the diagnosis of pilomatricoma. Dermoscopy may be a useful tool for improving the clinical recognition of pilomatricoma.
Key words: Dermoscopy; Pilomatricomas; Adnexal tumor
INTRODUCTION
Pilomatrixoma is a benign adnexal, dermal, or subcutaneous tumor [1].
The tumor was first described by Malherbe and Chenantais in 1880, who hypothesized that the lesion originated from a sebaceous gland and, therefore, they named the tumor calcifying epithelioma of sebaceous glands [2,3].
The lesion usually occurs on the face, neck, and upper limbs, while the trunk and the lower limbs are less often affected [4].
Typically, pilomatricoma is described as a firm, painless, well-defined solitary nodule, which may have a bluish-red coloration. Its size normally ranges from 0.5 to 4.5 cm in diameter and the highest incidence is found in children and females [5].
Dermoscopy is a non-invasive technique that has greatly improved the diagnostic accuracy of melanocytic and non-melanocytic skin tumors.
We present the dermoscopic features of pilomatricoma through our case report with a literature review.
CASE REPORT
An eleven-year-old female was admitted to our department for a rapidly-growing, painless tumor of the back which had been evolving for four months. There was no notion of prior trauma nor a tendency for spontaneous regression.
A clinical examination revealed an erythematous-purplish tumor 3 cm in diameter with a smooth and telangiectatic surface. The tumor was roughly rounded, adhered to the superficial planes, and painless on palpation (Fig. 1).
 |
Figure 1: Erythematous-violaceus tumor in the back of the eleven-year-old female. |
Dermatoscopic examination of the lesion showed structures invisible to the naked eye. There were multiple irregular, yellowish-white structures, white streaks, yellowish lobules, blueish-gray areas, and linear, irregular vessels (Figs. 2 and 3).
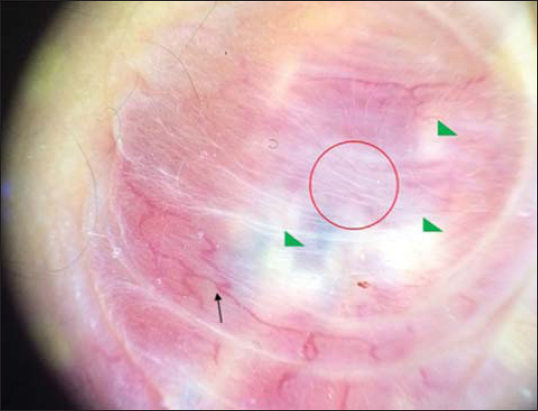 |
Figure 2: Dermoscopy of pilomatricoma (red circle: white streaks; black arrow: linear-irregular vessels; green triangles: structureless yellow-whitish areas). |
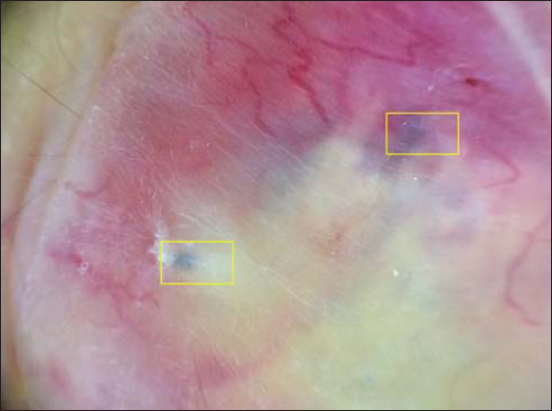 |
Figure 3: Dermoscopy of pilomatricoma (chunks: structureless bluish-gray areas). |
Histological examination of the excised specimen revealed a dermal tumor made of several rounded masses, the largest having a cystic appearance. In the most superficial zone, there were numerous ghost cell ranges. There were also intensely dark, matrix-like basophilic cell areas with characteristic maturation toward eosinophilic transitional cells and then nucleus-free ghost cells. Mummified cells were sometimes calcified and surrounded by zones of foreign body granuloma.
Thus, the diagnosis of pilomatricoma clinically and dermoscopically suspected was confirmed by histology.
DISCUSSION
Pilomatricoma is a common tumor derived from hair matrix cells; it is most often diagnosed in young children yet may also affect adults [6].
It clinically presents itself as a firm, single, stony-hard, slow-growing subcutaneous or intradermal nodule, asymptomatic and adherent to the skin. Lesions are usually skin-colored, although reddish-blue lesions have also been observed [7].
Dermoscopy is a non-invasive procedure focusing on analyzing epidermal and dermal structures, although it is widely used to facilitate the diagnosis of melanocytic and non-melanocytic skin lesions [1].
Since 2008 till now, dermoscopic features of fifteen cases of pilomatricomas have been reported in published English-language works, including our case (Table 1).
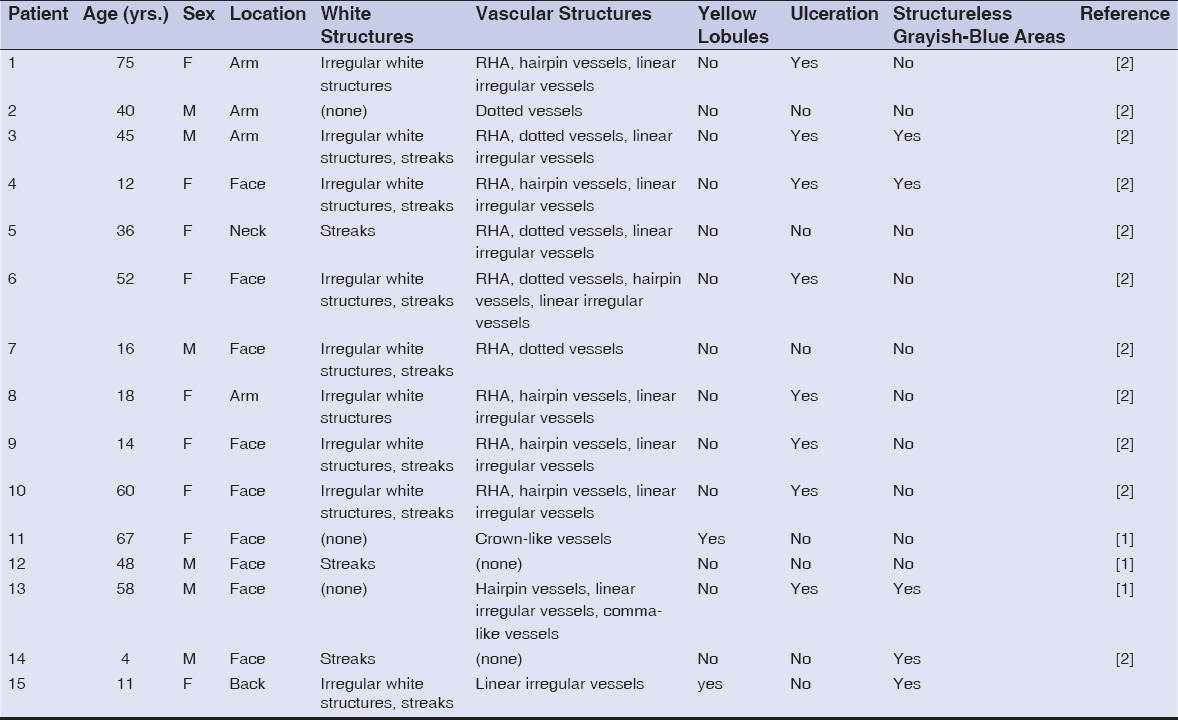 |
Table 1: Summary of the cases of pilomatricoma with dermoscopic features (F: female; M: male; RHA: reddish homogeneous area) |
The patients, nine females and six males, were aged from 4 to 75 years old (mean = 37.06). Nine of the lesions (60%) were located on the face, four (26,66%) on the upper extremities (arm), and the two (13,3%) remaining were located one (6,67%) on the back and the other on the neck (6,67%) [1–2].
A dermoscopic examination of the lesions allowed the observation of the following features: white streaks and irregular yellow-whitish structures were present in nine pilomatricomas (60%); vascular structures were identified in thirteen cases (86.66%); reddish homogeneous areas, linear-irregular vessels, and hairpin-like vessels were observed in nine cases (60%); dotted vessels in four cases (26,7%), and crown-like vessels and comma-like vessels in one case (6.7%); ulceration was observed in eight pilomatricomas (53.3%); structureless grayish-blue areas were found in five cases (33.3%); and yellowish lobules were found in two cases (13.3%) [1–2].
The diagnosis of pilomatricoma was confirmed histologically in our case and those in other reports by showing a well-circumscribed, deep-dermal or dermal-subcutaneous tumor formed by basaloid cells that gradually lost their nuclei and mingled with the eosinophilic shadow cells that showed ghosts of epithelial cells. Calcification may be seen in shadow cell regions along with a foreign-body giant-cell reaction to keratin [1,2].
The correlation between dermoscopic and histologic features of pilomatricoma was reported by Pedro Zallos et al. [2]:
- Irregular yellow-whitish structures and streaks correspond histologically to the presence of calcification but also to large masses of eosinophilic cornified material located in the center of the well-developed lobules of pilomatricoma.
- The reddish homogeneous area may be attributed to the presence of numerous proliferating vessels located in the papillary dermis and the presence of hemorrhage.
- The small structureless grayish-blue areas correspond histologically to melanin pigment within aggregates of basaloid cells or the presence of siderophages or melanophages in the inflammatory infiltrate.
Thus, the diagnosis of pilomatricoma was suspected in 90% of cases with the help of dermoscopy, in the absence of specific criteria for other cutaneous tumors, and in front of the presence of irregular white structures associated with vascular structures [2].
CONCLUSION
The current report described the dermoscopic features of pilomatricoma. However, the number of cases is insufficient to study the sensibility and specificity of each dermoscopic feature.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Ayhan E, Ertugay O, Gundogdu R. Three different dermoscopic view of three new cases with pilomatrixoma. Int J Trichology. 2014;6:21-2.
2. Wolff CR, Brehmer F, Lockmann A, Hofmann L, Brauns B, Schön MP, et al. Rapidly growing blue-red nodule on the cheek of a 4-year-old boy. J Dtsch Dermatol Ges. 2014;12:432-4.
3. Taoufi KN, El Ouatassi N, Bamine H, El Alami El Amine NM, El Kadiri S, Baybay H, et al. Proliferating pilomatrixoma mimicking squamous cell carcinoma. Our Dermatol Online. 2021;12(e):e4.
4. Han G, Kim AR, Song HJ, Oh CH, Jeon J. Updated view on epidemiology and clinical aspects of pilomatricoma in adults. Int J Dermatol. 2017;56:1032-6.
5. Pinheiro TN, Fayad FT, Arantes P, Benetti F, Guimarães G, Cintra LTA. A new case of the pilomatrixoma rare in the pre-auricular region and review of series of cases. Oral Maxillofac Surg. 2018;22:483-8.
6. Corredor-Osorio R, Suarez-Tata M, Orellana ME. Pilomatricoma of the orbit. Our Dermatol Online. 2016;7:188-90.
7. Inamura Y, Hata H, Imafuku K, Kitamura S, Shimizu H. Would you consider pilomatricoma as a differential diagnosis?Our Dermatol Online. 2016;7:117-8.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0002-0905-4908 http://orcid.org/0000-0002-0905-4908 |

Comments are closed.