Facial actinic lichen nitidus in a geriatric Tunisian female
Khaoula Ameur 1, Yosra Soua1, Leila Njim2, Hichem Belhadjali1, Monia Youssef1, Jameleddine Zili1
1, Yosra Soua1, Leila Njim2, Hichem Belhadjali1, Monia Youssef1, Jameleddine Zili1
1Department of Dermatology, Fattouma Bourguiba University Hospital, Monastir, Tunisia, 2Department of Anatomopathology, Fattouma Bourguiba University Hospital, Monastir, Tunisia
Corresponding author: Dr. Khaoula Ameur
Submission: 10.12.2019; Acceptance: 11.02.2020
DOI: 10.7241/ourd.20204.9
Cite this article: Ameur K, Soua Y, Njim L, Belhadjali H, Youssef M, Zili J. Facial actinic lichen nitidus in a geriatric Tunisian female. Our Dermatol Online. 2020;11(4):371-372.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Actinic lichen nitidus (ALN) is an unusual variant of lichen nitidus (LN) appearing only on photo-exposed areas. It is usually seen in deeply pigmented adult and pediatric patients with a history of significant sun exposure during the summer months. We report an atypical case of facial ALN in a geriatric Tunisian female with a one-year history of facial pruritic lesions marked during the summer months. A histologic examination was suggestive of lichen nitidus, and the diagnosis of ALN was reached. ALN is a photoinduced lichenoid eruption that shows the classical histologic features of lichen nitidus with a degree of clinical similarity. Only five cases of exclusively facial lesions have been reported. This type of dermatosis occurs commonly in pediatric patients and young adults. ALN affects preferentially individuals of darker skin tones. Only one case of ALN in a patient of a lower Fitzpatrick skin phototype, as our case, had previously been reported.
Key words: Lichenoid Eruptions, Lichen nitidus
INTRODUCTION
Lichen nitidus (LN) is an inflammatory skin disorder most commonly occurring in children. Its etiology remains unknown [1]. Actinic lichen nitidus (ALN) is an unusual variant of LN that appears only on photo-exposed areas [2]. It is usually seen in deeply pigmented adult and pediatric patients with a history of significant sun exposure during the summer months [2–4]. It was previously reported as a summertime actinic lichenoid eruption and lichen nitidus actinicus [4]. This entity appears to be an underrecognized disease in the north of Africa [4]. We report an atypical case of facial ALN in a geriatric Tunisian female.
CASE REPORT
A 62-year-old Tunisian female presented herself at our Dermatology Department with a one-year history of facial pruritic lesions marked during the summer months. A physical examination revealed numerous symmetrically distributed, flesh-colored, shiny papules associated with brownish erythematous plaques on the forehead, cheeks, nose, and chin, sparing the frontal hairline, vertical forehead folds, nasolabial folds, upper eyelids, and the area of the upper lip shaded by the nose. The patient’s Fitzpatrick phototype was III (Fig. 1). The rest of the examination—mainly of the hair, nails, and mucosas—were normal. A histological examination revealed a dense granulomatous lichenoid infiltrate filling the papillary dermis and being bordered by elongated epidermal rete ridges in a “ball-in-a-claw” pattern. The epidermis was slightly thinned with an orthokeratotic stratum corneum and focal parakeratosis (Fig. 2). This aspect was suggestive of LN. The patient was treated with topical corticosteroids and photoprotection with partial remission.
 |
Figure 1: Multiple shiny flesh-colored papules associated with brownish erythematous plaques distributed on the face. |
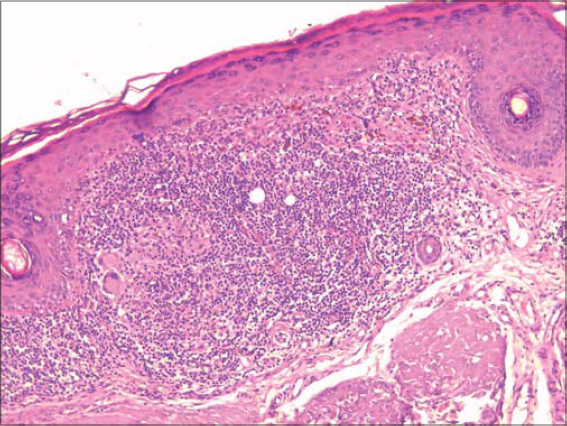 |
Figure 2: A dense granulomatous lichenoid infiltrate embraced by rete ridges under a thinned epidermis (H&E, 200×). |
DISCUSSION
ALN is a photoinduced lichenoid eruption that shows the classical histologic features of lichen nitidus with a degree of clinical similarity. It appears only on photo-exposed areas [2]. It was first reported in India in 1978 by Bedi, who described 25 patients with hypopigmented pinpoint papules in sun-exposed areas and named the entity a summertime actinic lichenoid eruption [5]. The term of ALN was proposed in 1991 by Kanwar et al., who described six children with this clinical presentation [6].
Since then, short series of patients with the same clinical presentation have been reported [2,3]. This dermatosis occurs commonly in pediatric patients and young adults. Most of the reported cases of ALN have described lesions on the forehead, dorsum of the hands, and the V area of the neck [7]. Only five cases of exclusively facial lesions have been reported [4,7].
ALN affects preferentially individuals of darker skin tones (Fitzpatrick skin types IV and V) from Africa, America, the Middle East, and India [2]. The only case of ALN in a patient of a lower Fitzpatrick skin phototype, as our case, was reported by Solano-Lopez in a Caucasian European patient [2]. The differential diagnosis includes actinic folliculitis, sarcoidosis, and mucinosis. The diagnosis of ALN is confirmed by a histopathological examination, which reveals the characteristic aspects of LN [3]: a dense, well-circumscribed, subepidermal infiltrate, sharply limited to one or two adjacent dermal papillae in a “ball-in-a-claw” pattern. Giant cells are sometimes present. A true granuloma may occasionally be found, although caseation is never present [5,6]. The treatment of ALN is based on local corticosteroids and photoprotection. One patient has been successfully treated with hydroxychloroquine [4].
CONCLUSION
This case highlights the existence of this entity in individuals of lower Fitzpatrick skin phototypes.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Chu J, Lam JM. Lichen nitidus. CMAJ. 2014;186):E688.
2. Solano-Lopez G, De Argila D, Fraga J, Dauden E. Actinic lichen nitidus in a Caucasian European patient. J Eur Acad Dermatol Venereol. 2014;28:1403-4.
3. Glorioso S, Jackson SC, Kopel AJ, Lewis V, Nicotri T, Jr. Actinic lichen nitidus in 3 African American patients. J Am Acad Dermatol. 2006;54(2 Suppl):S48-9.
4. Bouras M, Benchikhi H, Ouakkadi A, Zamiati S. Facial actinic lichen nitidus successfully treated with hydroxychloroquin:a case report. Dermatol Online J. 2013;19:20406.
5. Bedi TR. Summertime actinic lichenoid eruption. Dermatologica. 1978;157:115-25.
6. Kanwar AJ, Kaur S. Lichen nitidus actinicus. Pediatr Dermatol. 1991;8:94-5.
7. Dar NR, Rao SU. Facial lichen nitidus actinicus. Australas J Dermatol. 2012;53:e16-7.
Notes
Source of Support: Nil.
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.