MYZAP a newly protein expressed in the skin is autoantigen for patients with endemic pemphigus foliaceus in El Bagre, Colombia
Ana Maria Abreu Velez 1, Yulieth Alexandra Upegui-Zapata2, Carlos Andres Valencia-Yepes3, Eduardo Upegui-Quiceno4, Hong Yi5, Michae S. Howard1
1, Yulieth Alexandra Upegui-Zapata2, Carlos Andres Valencia-Yepes3, Eduardo Upegui-Quiceno4, Hong Yi5, Michae S. Howard1
1Georgia Dermatopathology Associates, Atlanta, Georgia, USA, 2PECET, PhD, Medical Research Institute, School of Medicine, University of Antioquia, Medellin, Colombia, South America, 3Undergraduated student, Department of Education, University of Antioquia, Medellin, Colombia, South America, 4PECET Programa de Estudio y Control de Enfermedades tropicales, Medical Research Institute, School of Medicine, University of Antioquia, Medellin, Colombia, South America, 5Robert P. Apkarian Integrated Electron Microscopy Core, Emory University Medical Center, Atlanta, GA, USA
Corresponding author: Ana Maria Abreu Velez, M.D., Ph.D, Dr.Sc
Submission: 02.07.2020; Acceptance: 07.07.2020
DOI: 10.7241/ourd.20204.2
Cite this article: Abreu Velez AM, Upegui-Zapata YA, Valencia-Yepes CA, Upegui-Quiceno E, Yi H, Howard MS. MYZAP a newly protein expressed in the skin is autoantigen for patients with endemic pemphigus foliaceus in El Bagre, Colombia. Our Dermatol Online. 2020;11(4):340-345.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Background: We detected autoantibodies against a new complex cell junction, the area composita of the heart [an intricate cell junction that includes the protein Myocardial Zonula Adherens Protein (MYZAP, AKA MYOZAP)] in patients affected by a new variant of endemic pemphigus foliaceus in El Bagre, Colombia, South America (El Bagre-EPF).
Methods: We aimed to study if MYZAP was expressed in the skin, and, if so, its relationship with El Bagre-EPF autoantigens. We utilized a case-control study, testing 43 patients and 43 controls from the endemic area matched by demographics, age, gender, living place, and work activities using multiple immunological methods.
Results: MYZAP is expressed in the human skin (epidermis and dermis), as well in the skin appendages, their neurovascular supply structures, and neural receptors (in all of these sites, mostly in the cells junctions). MYZAP present in the cell membranes, and is also located in intracytoplasmic and nuclear regions. All El Bagre-EPF patient autoantibodies perfectly colocalized with MYZAP (a commercial antibody from Progen Biotechnik, Heidelberg, Germany) in the skin (p< 0.01).
Conclusion: We describe for the first time in the medical literature the expression of a new protein MYZAP in several structures in the skin, colocalizing with El Bagre-EPF autoantigens and suggesting that further studies could focus on the putative roles of this molecule in the skin.
Key words: Endemic pemphigus foliaceus in El Bagre, MYZAP, skin, cells junctions
Abbreviations: Endemic pemphigus foliaceus (EPF), endemic pemphigus foliaceus in El Bagre (El Bagre-EPF), fogo selvagem (FS), hematoxylin and eosin (H&amp;E), immunofluorescence (DIF), immunohistochemistry (IHC), confocal microscopy (CFM), basement membrane zone (BMZ), intercellular stain between keratinocytes (ICS), The intercalated disc (ID), adherens junctions (AJ), desmoglein 1 (Dsg1), Myocardial Zonula Adherens Protein (MYZAP), (glutamate ionotropic receptor N-methyl-D-aspartate receptor type subunits (GRINL1A), adherens junctions (AJs), the intercalated disk (ID), serum response factor (SRF), The ionotropic glutamate N-methyl D-aspartate (NMDA), fluorescein isothiocyanate (FITC).
INTRODUCTION
Endemic pemphigus foliaceus (EPF) provides a superb model to study autoimmune diseases, given its geographic and family clustering, immune response, patient genetics and putative triggering factor(s) [1–9]. EPF is seen in South America, Central America, as well as in Tunisia, Africa [6] and it has a genetic component, as well as putative triggering factors [1–10]. El Bagre-EPF is an autoimmune disease that has several clinical forms including a form frustre (localized to the skin, mostly of the face and upper chest), and a spectrum of more extensive involvement including presentations resembling Senear-Usher syndrome and a systemic form affecting multiple organs [11–15].
Our recent studies indicated colocalization of the El Bagre-EPF autoantibodies with the Myocardial Zonula Adherens Protein (MYZAP) (AKA MYOZAP), in the area composita of the heart, in its conductive system, and in vessels [11]. Given the fact that El Bagre-EPF patients have autoantibodies to MYZAP in the cardiovascular system, we aimed to search for the expression of MYZAP in the skin and, if present, for any relationship with El Bagre-EPF autoantibodies.
MATERIALS AND METHODS
Patients
A human quality assurance review board approved the studies at the Hospital Nuestra Señora del Carmen in El Bagre. All participants signed informed consent forms. We tested 43 patients with El Bagre-EPF and 43 healthy controls from the endemic area, matched by age, gender, demographics (including history of malaria, gastrointestinal infections or sexually transmitted diseases, dengue, tuberculosis; cohabitation with domestic animals; exposure to wild animals, living and working activities, distance to rivers; tobacco, marijuana or liquor habits; exposure to agricultural and jungle vegetation; exposure to rodents, mosquitoes, and snakes and other jungle animals during rest or work hours; basic diet, and employment activities). The patients were evaluated clinically, and biopsy samples were assessed by hematoxylin and eosin (H&amp;E) staining, by direct immunofluorescence (DIF), immunohistochemistry (IHC), confocal microscopy (CFM), ELISA, immunoblotting (IB) and immunoprecipitation (IP), and indirect inmunoelectron microscopy (IEM) as previously described [3–5,8–10]. For DIF, biopsies were taken from perilesional skin on the chest; control biopsies were also obtained from the chest. For the IIF, the skin samples were obtained from cadaver donors with a proper Institutional Review board permit.
Patients were included only after these tests were performed and if they fulfilled the following full diagnostic criteria for El Bagre-EPF: (i) the patient presented the clinical and epidemiological features described for this disease; (ii) they lived in the endemic area; (iii) their serum displayed intercellular staining between epidermal keratinocytes by DIF and to the basement membrane zone of the skin, using fluorescein isothiocyanate (FITC)-conjugated monoclonal antibodies to human total IgG or to IgG4, as previously described; [3–5] (iv) their serum was positive by IB for reactivity against desmoglein 1 (Dsg1) and plakin molecules, as previously described [4,5], (v) their serum immunoprecipitated a Concanavalin A affinity-purified antigen bovine tryptic 45 kDa fragment of desmoglein 1 (Dsg1) [8]; and (vi) the patient serum yielded a positive result using an ELISA when screening for autoantibodies to pemphigus foliaceus (PF) antigens [9].
DIF and IIF Studies
Our studies were performed as previously described [3–5,7–10]. The slides were counterstained with 4,6-diamidino-2-phenylindole (Pierce, Rockford, IL, USA). We also used antibodies to a mouse monoclonal antibody for myocardium-enriched zonula occludens-1-associated protein (Myozap; Progen Biotechnik, Heidelberg, Germany, Cat no. 651169). For the secondary antibody to MYZAP, we utilized Texas red-conjugated goat anti-mouse IgG (Thermo Fisher Scientific, Waltham, MA). All samples were consistently run with positive and negative controls. We classified our findings as negative (-), weakly positive (+/-), positive (++) and strongly positive (+++) [3–5].
Confocal Microscopy (CFM)
Colocalization of the patient’s autoantibodies with commercial antibodies was confirmed using CFM. Our CFM studies were performed as previously described [11–15]. In brief, we utilized standard 20X and 40X objective lenses; each photoframe included an area of approximately 440 x 330 µm. Images were obtained using EZ-1 image analysis software (Nikon, Tokyo, Japan). For colocalization experiments with serum autoantibodies, we used the previously described antibodies to MYZAP [16].
Indirect immunoelectron microscopy (IEM)
Our technique was performed as previously described [11]. Postembedding immunogold labeling was performed on samples, and human skin was used as an antigen. The tissue was fixed in 4% glutaraldehyde with 0.2% paraformaldehyde, and embedded in Lowicryl® resin. Sections of 70 nm thickness were cut and blocked; the grids were then washed, and the primary antibody was incubated, washed, and a secondary antibody solution, specifically 10 nm Gold-conjugated protein A PBS-BSAC (Aurion, EMS™) was applied [11–15]. The samples were then double-stained with uranyl acetate and lead citrate, and observed under a Hitachi H7500 transmission electron microscope. Immunogold particle images displaying any pattern of positivity were then converted to TIF format as previously described [11–15].
Statistical Analysis
We used Fisher’s exact test to compare two nominal variables (e.g. positive and negative) of the antibody response. We also compared the differences when evaluating: (i) positivity of the El Bagre EPF autoantibodies between patient cases and controls; and (ii) patient antibody results versus the commercial antibodies to MYZAP. A p < 0.01 with 98% confidence or more was considered statistically significant. We used GraphPad QuickCalcs software from GraphPad Software (La Jolla, CA, USA).
RESULTS
DIF, IIF, CFM and IEM studies showed that MYZAP is expressed in human skin epidermis, dermis, and the basement membrane zone (BMZ); this was noted in all the El Bagre EPF patient cases and all the controls, indicating that MYZAP is widely expressed in the skin and is a constitutive protein (p< 0.01). Using DIF and CFM, the MYZAP commercial antibody perfectly colocalized with the autoantibodies from patients affected by El Bagre-EPF in the skin in 98% of the cases (p< 0.01) (Table 1). There was no positive colocalization with MYZAP in any of the matched control individuals.
 |
Table 1: DIF data documenting expression and positivity of El Bagre-EPF patient autoantibodies in chest skin, and respective colocalizations with MYZAP |
In El Bagre-EPF patients autoantibodies and their colocalization with MYZAP were clearly appreciated using DIF and CFM, and both techniques revealed that cell junctions were positive in 98% of the cases (p< 0.01). The cells junctions were positive in the epidermis, and the BMZ as well as in all skin appendices and their neurovascular supplies. At higher magnifications, the MYZAP locations were observed at the plasma membranes (including both cell and nuclear). MYZAP was also in observed intracytoplasmic and intra-nuclear locations in the epidermal cells in 98% of the cases (p< 0.01). In the dermis, the mesenchymal endothelial cell junctions were also positive for MYZAP, colocalizing with the El Bagre-EPF autoantibodies (p < 0.01). Of interest, the neurovascular bundles in both the upper and lower dermis were strongly positive for MYZAP as well as all free and encapsulated skin neural receptors; these sites also demonstrated colocalization with El Bagre-EPF autoantibodies (Figs. 1 and 2).
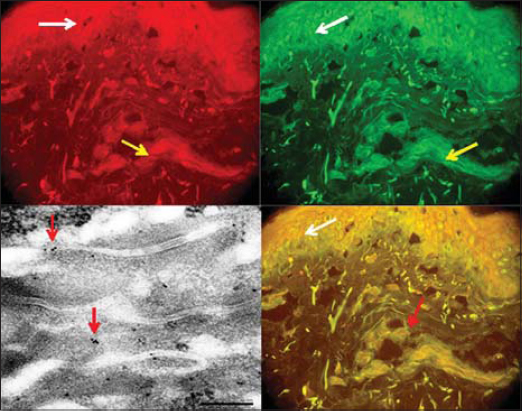 |
Figure 1: Confocal microscopy data is presented in the upper left, upper right and lower right images). Upper left, red being expressed in the entire skin including the epidermis (white arrow) (with strongest expression in the corneal and granulosum layers; 200X). MYZAP is also expressed in the basement membrane zone, and in the dermis including both the superficial and deep neurovascular plexuses (yellow arrow). The upper right panel shows the positivity of the El Bagre-EPF autoantibodies using anti-IgG FITC conjugated showing in green the stain in the epidermis (white arrow), and in the vessels (yellow arrow) (200X). The lower right figure shows a confocal image of both MYZAP and El Bagre-EPF autoantibodies perfectly colocalizing in the epidermis (white arrow), as well as in the dermis (red arrow) (200X). The lower left panel using IEM data demonstrating positive staining for MYZAP in skin epidermal cell junctions IEM photographs of patient skin, showing MIZAP antibodies labelled with 10 nm Gold-conjugated protein A antibodies (tiny black dots). The antibodies are located in the epidermal cells junctions (red arrows), (100kV). |
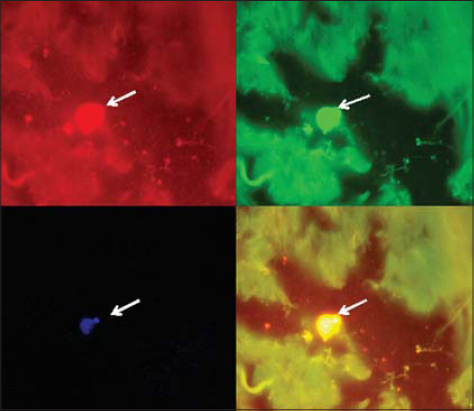 |
Figure 2: A confocal image shows a four panel figures. In the upper left panel we observe the positivity of a nucleated neural dermal receptor stained with DAPI (white arrow) (400X). In the upper right figure we observed a positive stain against a skin dermal receptor showing the positivity of the El Bagre-EPF autoantibodies using anti-IgG FITC conjugated in green the stain (white arrow), (400X). In the left lower panel we show a positive stain using the Myzap Texas red conjugated antibody against a dermal neural receptor (white arrow) (400X). In the lower right panel we show colocalization of DAPI, the patient’s autoantibodies and MYZAP being positive to the dermal neural receptor (white arrow), (400X). |
Using the indirect immunoelectron microscopy, MYZAP was mostly located at the cell junctions of the epidermis (Fig. 1).
Table 1 shows detailed results of DIF on chest skin from El Bagre-EPF patients. As shown, in the autoimmune response was polyclonal.
DISCUSSION
In this study, we demonstrated for the first time the presence of the protein MYZAP in the skin (and confirmed MYZAP as a new El Bagre-EPF autoantigen). MYZAP was originally titled MYOZAP (Myocardium-enriched Zo-1-interacting Protein), and designated as a novel intercalated disc protein (ID) [16]. In this study we demonstrate that MYZAP is expressed in the skin at multiple sites, mostly at cell junctions.
MYZAP has been shown to be strongly expressed in human heart, lung and skeletal muscle; in cardiac tissue, it localizes to the ID and directly binds to desmoplakin (another El Bagre-EPF autoantigen). It has been shown that in the heart that MYZAP bind to myosin phosphatase-RhoA interacting protein, a negative regulator of Rho activity with additional intracellular signal transduction functions [17].
It is important to note that the skin and the heart share numerous molecules; these are often altered in cardiocutaneous syndromes [18]. Of interest, many molecules expressed in the heart are also El Bagre-EPF antigens including desmoplakins 1 and 2, p0071 and ARVCF [13–15].
In vivo, knockout studies of the MYZAP protein in zebrafish lead to contractile dysfunction and cardiomyopathy. MYZAP is a 54-kD protein, not a member of any of the recognized cytoskeletal and junctional protein multigene families; it is a component of the plaques of the composite junctions in the ID connecting the cardiomyocytes of mammalian hearts [17]. MYZAP has one conserved domain; specifically, metal ion transporter CorA-like (MIT CorA-like), a divalent cation transporter in superfamily cl00459 at the genetic location 267 → 358 (See supplemental Table 1) [18,19] .
MYZAP has been also identified as a novel major component of adhering junctions in endothelia of the blood and the lymphatic vascular systems [20]. El Bagre-EPF autoantibodies also recognize these structures. More specifically, MYZAP is a primary constituent of the cytoplasmic plaques in the adherens junctions (AJ); it links endothelial cells of the mammalian blood and lymph vascular systems, including the desmoplakin-containing complexus adhaerentes of the virgultar cells of the lymph node sinus [17]. We previously demonstrated that in the heart (including its conducting system), neurovascular system and the optic nerve envelope, MYZAP colocalizes with El Bagre-EPF autoantibodies [13,14]. We also previously documented that MYZAP is expressed in the kidney (also colocalizing with El Bagre-EPF autoantibodies) [15].
Other monikers for MYZAP include glutamate ionotropic receptor N-methyl-D-aspartate receptor type subunits (GRINL1A), Upstream Protein, Gup, Myocardium-Enriched ZO1-Associated Protein, and Myocardial Intercalated Disc Protein [21]. MYZAP in the heart directly binds to and/or colocalizes with other key ID components including β-catenin, N-cadherin, plakophilin-2, desmoplakin and zonula occludens, and also binds to Dysbindin [17].
The MYZAP gene has been reported to be part of the ionotropic glutamate N-methyl D-aspartate receptor [21]. This is a glutamate receptor and ion channel (via gated ions) protein found in nerve cells; it is activated when glutamate and glycine bind to it. When activated, it allows positively charged ions to flow through the cell membrane [21].
Recently, genome-wide association studies of atrial fibrillation using non-coding, low-frequency coding and splice variant MYZAP genes were associated with disease risk through unknown mechanisms [22]. Based on this study and our previous studies showing that MYZAP is part of the heart conducting system, and given that El Bagre-EPF patients suffer cardiac rhythmic problems, MYZAP is likely of great importance to normal heart rhythm. Normal cardiac rhythm is modulated via the neural system and electrical impulses; we wonder if this molecule and its cell junction partners may play a similar synaptic role in the skin and other organs. Further studies could focus on complex putative roles beyond the cell junctions, as previously documented for selected retinal gap junctions [23].
We also suggest that this new El Bagre-EPF autoantigen may provide a conceptual framework to understand the breakdown of self-tolerance, if indeed such modifications are present in this autoimmune disease.
In conclusion, we describe for the first time the presence of MYZAP in the skin with multiple localizations, and further colocalizing with El Bagre-EPF patient autoantibodies. Further studies are needed to study potential utility in monitoring disease development and treatment, via roles in etiology and pathophysiology. Based on the location of this protein in our study, the function of MYZAP in the skin seems to be related to cell junctions. However, as with MYZAP in the heart, the functions of the molecule in the skin need to be further elucidated.
Acknowledgement
To the patients and El Bagre community.
Statement of Ethics
Our patient gave informed consent. Although Institutional Review Board (IRB) approval for a case report is not needed, the US Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule restricts how protected health information (individually identifiable health information) on any patient may be made. Compliance with patient privacy, institutional rules, and federal regulations were followed. No photos or illustrations that contain identifiable features are included in the case report, and the case(s) described in the report are not so unique or unusual that it might be possible for others to identify the patients.
REFERENCES
1. Abréu-Vélez AM, Reason IJ, Howard MS, Roselino AM. Endemic pemphigus foliaceus over a century:Part I. N Am J Med Sci. 2010;2:51-59.
2. Abréu-Vélez AM, Reason IJ, Howard MS, Roselino AM. Endemic pemphigus foliaceus over a century:Part II. N Am J Med Sci. 2010;2:114-25.
3. Abreu-Velez AM, Hashimoto T, Bollag W, Arroyave ST, Abrèu-Velez CE, Londoñoet ML, al. A unique form of endemic pemphigus in Northern Colombia. J Am Acad Dermatol. 2003;49:599-8.
4. Abrèu-Velez AM, Beutner EH, Montoya F, Bollag WB, Hashimoto T. Analyses of autoantigens in a new form of endemic pemphigus foliaceus in Colombia. J Am Acad Dermatol. 2003;49:609-14.
5. Hisamatsu Y, Abreu Velez AM, Amagai M, Ogawa MM, Kanzaki T, Hashimoto T. Comparative study of autoantigen profile between Colombian and Brazilian types of endemic pemphigus foliaceus by various biochemical and molecular biological techniques. J Dermatol Sci. 2003.32:33-41.
6. Morini JP, Jomaa B, Gorgi Y, Saguem MH, Nouira R, Roujeau JC, et al. Pemphigus foliaceus in young women. An endemic focus in the Sousse area of Tunisia. Arch Dermatol. 1993;129:69-73.
7. Abreu-Velez AM, Robles EV, Howard MS. A new variant of endemic pemphigus foliaceus in El-Bagre, Colombia:the Hardy-Weinberg-Castle law and linked short tandem repeats. N Am J Med Sci. 2009;1:169-78.
8. Abréu-Vélez AM, Javier Patiño P, Montoya F, Bollag WB. The tryptic cleavage product of the mature form of the bovine desmoglein 1 ectodomain is one of the antigen moieties immunoprecipitated by all sera from symptomatic patients affected by a new variant of endemic pemphigus. Eur J Dermatol. 2003;13:359-66.
9. Abréu-Vélez AM, Yepes MM, Patiño PJ, Bollag WB, Montoya F Sr. A sensitive and restricted enzyme-linked immunosorbent assay for detecting a heterogeneous antibody population in serum from people suffering from a new variant of endemic pemphigus. Arch Dermatol Res. 2004;295:434-41.
10. Howard MS, Yepes MM, Maldonado-Estrada JG, Villa-Robles E, Jaramillo A, Botero JH, et al. Broad histopathologic patterns of non-glabrous skin and glabrous skin from patients with a new variant of endemic pemphigus foliaceus (Part 1). J Cutan Pathol. 2010;37:222-30.
11. Abreu-Velez AM, Zhe J, Howard MS, Gao W, Yi H, Grossniklaus HE, et al. Cardiac autoantibodies from patients affected by a new variant of endemic pemphigus foliaceus in Colombia, South America. J Clin Immunol. 2011;31:985-97.
12. Abreu Velez AM, Howard MS, Velázquez-Velez JE. Cardiac rhythm and pacemaking abnormalities in patients affected by endemic pemphigus in Colombia may be the result of deposition of autoantibodies, complement, fibrinogen, and other molecules. Heart Rhythm. 2018;15:725-31.
13. Abreu-Velez AM, Howard MS, Yi H, Gao W, Hashimoto T, Grossniklaus HE. Neural system antigens are recognized by autoantibodies from patients affected by a new variant of endemic pemphigus foliaceus in Colombia. J Clin Immunol. 2011;31:356-68.
14. Abreu Velez AM, Yi H, Warfvinge G, Howard MS. Autoantibodies to full body vascular cell junctions colocalize with MYZAP, ARVCF, desmoplakins I and II and p0071 in endemic pemphigus in Colombia, South America. Int J Dermatol. 2018;57:291-98.
15. Abreu-Velez AM, Howard MS, Yi H, Florez-Vargas AA. Patients affected by a new variant of endemic pemphigus foliaceus have autoantibodies colocalizing with MYZAP, p0071, desmoplakins 1-2 and ARVCF, causing renal damage. Clin Exp Dermatol. 2018;43:692-2.
16. Seeger TS, Frank D, Rohr C, Will R, Just S, Grund C, et al. Myozap, a novel intercalated disc protein, activates serum response factor-dependent signaling and is required to maintain cardiac function in vivo. Circ Res. 2010;106:880-90.
17. Bardawil T, Khalil S, Bergqvist C, Abbas O, Kibbi AG, Bitar F, et al. Genetics of inherited cardiocutaneous syndromes:a review. Open Heart. 2016;22;3:e000442.
18. https://www.omim.org/entry/614071 (consulted on June 17, 2020).
19. Pieperhoff S, Rickelt S, Heid H, Claycomb WC, Zimbelmann R, Kuhn C, et al. The plaque protein myozap identified as a novel major component of adhering junctions in endothelia of the blood and the lymph vascular systems. J Cell Mol Med. 2012;16:1709-19.
20. https://www.ncbi.nlm.nih.gov/gene/100820829 (accessed 06/07/2020).
21. Roginski RS, Goubaeva F, Mikami M, Fried-Cassorla E, Nair MR, Yang J. GRINL1A colocalizes with N-methyl D-aspartate receptor NR1 subunit and reduces N-methyl D-aspartate toxicity. NeuroReport. 2008:19:1721-6.
22. Thorolfsdottir RB, Sveinbjornsson G, Sulem P, Nielsen JB, Jonsson S, Halldorsson GH, et al. Coding variants in RPL3L and MYZAP increase risk of atrial fibrillation. Commun Biol. 2018;1:68.
23. O’Brien J, Bloomfield SA. Annu Rev Vis Sci. 2018:79-80.
Notes
Source of Support: Nil.
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0002-7692-4133 http://orcid.org/0000-0002-9348-6227 http://orcid.org/0000-0003-0430-6093 http://orcid.org/0000-0002-7692-4133 http://orcid.org/0000-0002-9348-6227 http://orcid.org/0000-0003-0430-6093 |

Comments are closed.