Elephantiasis neuromatosa
Giuseppe Famularo 1, Laura Conversano1, Liborio Manente2
1, Laura Conversano1, Liborio Manente2
1Internal Medicine, San Camillo Hospital, Rome, Italy; 2Pathology, San Camillo Hospital, Rome, Italy
Corresponding author: Dr. Giuseppe Famularo, E-mail: g.famularo@icloud.com
Submission: 25.06.2019; Acceptance: 27.07.2019
DOI: 10.7241/ourd.20201.13
Cite this article: Shah FY, Bhat YJ, Zeerak S, Wani R, Hassan Shah I. Cutaneous mastocytosis mimicking hypertrophic scars: A case report. Our Dermatol Online. 2020;11(1):50-52.
Citation tools:
BibTex | CSV | RIS | Endnote XML
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Elephantiasis neuromatosa is usually associated with NF-1 mutation and sporadic cases are very rare. A 75-year-old woman presented with growing masses involving the left leg. A physical examination revealed an enlarged left leg with more than 30 huge, hard, and firm nodules below the knee. A biopsy specimen of a nodule showed a soft-tissue neurofibroma. The patient refused to undergo surgical de-bulking and was subsequently lost to follow-up. Our case had no personal or family history of neurofibromatosis type 1 and no other features of the disorder were recognized. There is agreement that, irrespective of the presence of NF-1 mutation, elephantiasis neuromatosa arises from a plexiform neurofibroma of the superficial and deep nerves ultimately leading to the elephant-like and grotesque appearance of the involved limb. Surgical de-bulking and limb amputation are needed in most severe cases.
Key words: Elephantiasis neuromatosa. Neurofibroma. von Recklinghausen phenotype. Lymphostasis
INTRODUCTION
Elephantiasis neuromatosa (EN) is characterized by abnormal soft-tissue hypertrophy and bone dysplasia that are associated with early and exaggerated bone growth of the affected leg along with the growth of infiltrating neurofibromas and lymphangiomatosis [1]. Thinning of bones, erosion of articular surfaces and periosteal dysplasia are other common features. A substantial proportion of cases are associated with neurofibromatosis type 1, i.e. the von Recklinghausen disease [1]. Sporadic patients have been reported even more rarely.
CASE REPORT
A 75-year-old woman had a one-year history of growing and painful masses involving the left leg. Previous history was remarkable for hypertension and chronic lymphedema of the lower limbs and her drug regimen consisted of ramipril and furosemide. A physical examination revealed an enlarged left leg with more than 30 huge, hard, and firm nodules below the knee. The nodules were up to 7 cm in maximum size, the overlying skin was thickened and pigmented, and no ulceration was seen (Figs. 1a and 1b). The right lower limb was normal. A biopsy specimen of a nodule of the left leg showed a soft-tissue neurofibroma (Fig. 2). The patient refused to undergo surgical de-bulking to alleviate the pain and improve the cosmetic appearance. She was treated conservatively and was subsequently lost to follow-up.
 |
Figure 1: (a and b) Severe hypertrophy of the left leg with several huge, hard, and firm nodules below the knee. The greatest nodule was up to 7 cm in maximum size. The overlying skin appeared thickened and pigmented, with no ulceration. |
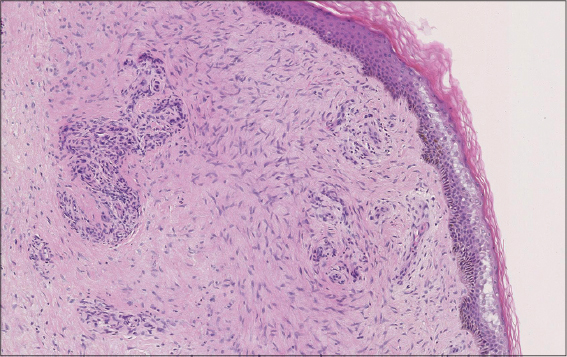 |
Figure 2: Histopathological examination (hematoxylin and eosin) of a sample from a nodule biopsy shows spindle cells arranged in short fascicles infiltrating the dermis and the underlying soft-tissues, a finding suggestive of a massive neurofi broma. |
DISCUSSION
At presentation, the findings in this patient were highly reminiscent of EN, a rare and very impressive disorder first described by Virchow, and well illustrate the typical features of this enigmatic disorder [2]. The underlying pathophysiology as well as the mechanistic pathways of EN are not fully understood particularly in the very rare sporadic cases who do not have the classical von Recklinghausen phenotype and in whom no NF-1 mutation is found. There is agreement that, irrespective of the presence of NF-1 mutation, EN arises from a plexiform neurofibroma of the superficial and deep nerves. The unregulated proliferation of the perineural connective, fat, muscle tissue, and bone is thought to play a major role and accounts for the locally aggressive behavior of the tumor even though there is no evidence of malignancy [3]. Ultimately, the unchecked growth of the neurofibroma and the paralleling exaggerated soft-tissue hypertrophy and bone dysplasia lead to the elephant-like and grotesque appearance of the involved limb. The disfiguring features of EN are usually limited to the lower third of the affected leg however the chest, buttocks and the limb roots can be also involved. Chronic lymphostasis, lymphedema, and the dysplasia and hyper-proliferation of the lymphatic vessels have been proposed to play a mechanistic role and consequently patients with chronic lymphedema and lymphostasis are at increased risk of developing EN as compared to healthy subjects [4]. This hypothesis fits well with the clinical presentation of our patient and her history of chronic lymphedema.
Most patients with EN have the NF-1 mutation [1]. Our case had no personal or family history of neurofibromatosis type 1 and no other features of the von Recklinghausen disease, such as “café au lait” spots, iris Lisch hamartomas, axillary and inguinal freckling, and skeletal abnormalities, were recognized. Filariasis, lymphangitis, cellulitis, and scleroderma are often advocated when first facing a patient with EN. However, a long-held dogma suggests that elephantiasis nostras verrucosa is the most important differential diagnosis for EN patients. Elephantiasis nostras verrucosa results from chronic venous stasis that triggers the appearance of chronic changes in areas of dependent edema such as hyperkeratosis, papillomatous plaques, loosely adherent crust and cobblestone-like nodules, erythema and skin ulcers [5].
Patients with EN may have infiltration of the subcutaneous fat and muscle compartments, which can cause severe muscle atrophy and functional impairment. Entrapment of the main limb veins and arteries is common and this can be an important cause of severe and potentially life-threatening bleeding. Ulceration and infection are other clinically relevant complications in the course of EN. Surgical de-bulking and limb amputation or disarticulation are needed in most severe cases of EN [6].
CONCLUSION
This patient presented with gross EN and massive gigantism of her left leg. The limb enlargement was extremely disfiguring and resulted in severe disability. In most cases, EN is a rare clinical manifestation of the von Recklinghausen disease and sporadic cases not associated with the NF-1 mutation are even more rare.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Ponti G, Pellacani G, Martorana D, Mandel VD, Loschi P, Pollio A, et al. Giant elephantiasis neuromatosa in the setting of neurofibromatosis type 1:a case report. Oncology Lett. 2016;11:3709-14.
2. Sullivan TP, Seeger LL, Doberneck SA, Eckardt JJ. Plexiform neurofibroma of the tibial nerve invading the median and lateral gastrocnemius muscles and plantaris muscle. Skeletal Radiol. 1994;23:149-52.
3. Bano S, Prasad A, Yadav SN, Chaudary V, Sachdeva N. Elephantiasis neuromatosa of the lower limb in a patient with neurofibromatosis type-1:a case report with imaging findings. J Pediatr Neurosci. 2010;5:59-63.
4. Lohrmann C, Pache G, Felmerer G, Foeldi E, Schaefer O, Langer M. Post-traumatic edema of the lower extremities:evaluation of the lymphatic vessels with magnetic resonance lymphangiography. J Vasc Surg. 2009;49:417-23.
5. Shah M. Elephantiasis nostras verrucosa. N Engl J Med. 2014;370:2520.
6. Hoshi M, Ieguchi M, Taguchi S, Yamasaki S. A case report of surgical debulking for a huge mass of elephantiasis neuromatosa. Rare Tum. 2009;1:e11.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.