|
Get Citation
|
|
|
Bouhajja L, Zaouak A, Koubaa W, Jannet SB, Hammami H, Fenniche S. Multiple brown nodules in an infant. Our Dermatol Online. 2019;10(1):56-58. |
|
|
Download citation file:
|
Multiple brown nodules in an infant
Leila Bouhajja1, Anissa Zaouak1, Wafa Koubaa2, Selima Ben Jannet1, Houda Hammami1, Samy Fenniche1
1Department of Dermatology, Habib Thameur Hospital, Tunis, Tunisia, 2Department of Pathology, Habib Thameur Hospital, Tunis, Tunisia
Corresponding author: Dr. Leila Bouhajja, E-mail: bouhaja.leila@gmail.com
Submission: 13.05.2018; Acceptance: 26.07.2018
DOI:10.7241/ourd.20191.14
ABSTRACT
Mastocytosis is a clonal disorder of mast cells. Systemic symptoms are typically a result of mast-cell mediator release. Urticaria Pigmentosa is the most common type of children mastocytosis. We report a case of a 9-month-old boy who presented for a widespread eruption since the age of 2 months. Physical examination revealed numerous red to brown slightely hyperpigmented papules and plaques on the trunk, the neck, the proximal upper and lower extremities and the genitalia. Complete blood count, hepatic and renal functions, abdominal ultrasonography were normal. A skin biopsy was performed and the histological exam confirmed the diagnosis of urticaria pigmentosa. The avoidance of chemical and physical stimuli was provided. He had only residual pigmentation at the lesional sites with no new lesion formation. The prognosis of childhood UP is good.
Key words: Mastocytosis, Urticaria Pigmentosa, Infant
INTRODUCTION
Mastocytosis is defined as a heterogeneous group of disorders characterized by an accumulation of mast cells in one or more organs, particularly in the skin, bone marrow, liver, spleen and lymph nodes [1]. Urticaria Pigmentosa (UP) is the most common presentation of cutaneous mastocytosis in children and represents 70-90% of the cases [2]. We report a new case of UP in a 9-month-old boy.
CASE REPORT
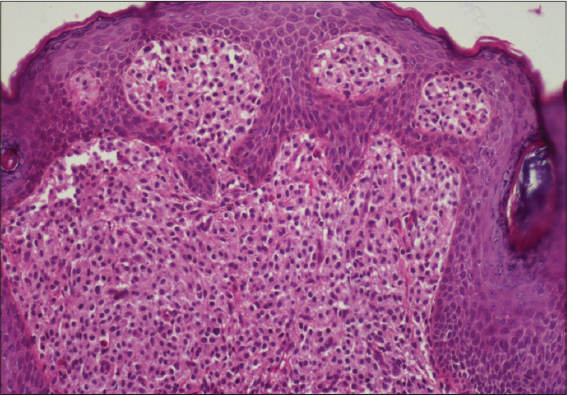
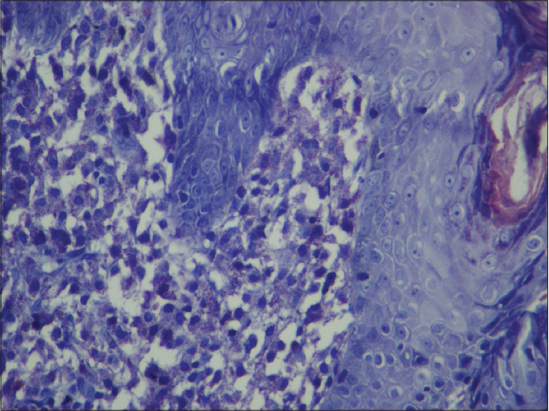
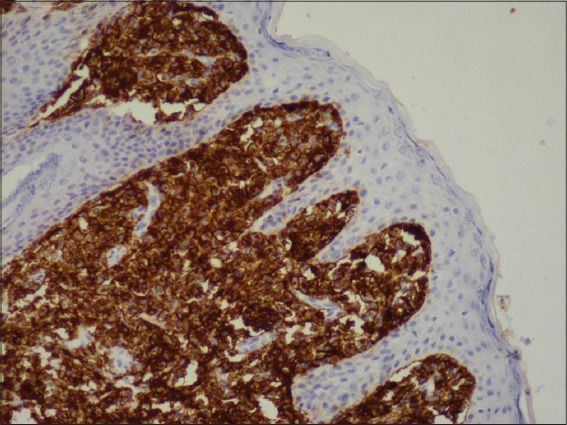
A healthy 9-month-old boy born at full term after an uncomplicated pregnancy, presented for a widespread eruption since the age of 2 months. He was otherwise, afebrile with a normal development. He was asymptomatic although sometimes some of his lesions became red and pruritic. There were no systemic symptoms such as flushing, vomiting, diarrhea, respiratory distress or irritability. Physical examination revealed a well-appearing infant. He had numerous red to brown slightely hyperpigmented papules and plaques on the trunk, the neck, the proximal upper and lower extremities and the genitalia (Fig. 1). There were no other skin lesions. Complete blood count, hepatic and renal functions, abdominal ultrasonography were all normal. A skin biopsy showed hyperpigmentation of the basal layer with dermal grouping of lymphocytes and mast cells (Fig. 2). The mast cells were identified with Giemsa staining and CD117 antibody (Figs. 3 and 4). The patient was regularly followed up in our department. General recommendations such as avoidance of chemical and physical stimuli were provided. He had only residual pigmentation at the lesional sites with no new lesion formation.

Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Urticaria pigmentosa (UP), also known as maculopapular mastocytosis, is the most common presentation of cutaneous mastocytosis in children and represents 70-90% of the cases [2]. Urticaria pigmentosa, is the most common form of mastocytosis disorder characterized by mast cell proliferation and accumulation within various organs, most commonly the skin. It is defined by multiple ovale or round red-brown hyperpigmented macules, papules, or nodules measuring a few mm to 1-2 cm in diameter. In 55% of patients, lesions appear before the age of 2 years, and in 10% of patients, it occurs between ages 2 and 15 years [3]. The affected areas include the trunk and extremities. The palms, soles, scalp and face are usually free of lesions [2]. The Darier’s sign is typically present. The pathogenesis of UP is unknown. Increased mast cell growth factors in skin lesions of UP are thought to stimulate mast cell proliferation, melanocyte proliferation and the production of melanin pigment. In addition, molecular studies demonstrated that UP is caused by several mutations in the KIT gene [4]. Histologically, the number of mast cells in the papillary dermis is increased. They are round or spindle shaped with abundant eosinophilic cytoplasm, distinct cytoplasmic boundaries, and large pale nuclei. They aggregate around blood vessels, and are sometimes associated with eosinophils. The basal layer is hyperpigmented. Nodular infiltrates extending to the subcutis may be seen, especially with special stains like toluidine blue and chloracetate esterase [5]. The treatment of UP is mainly symptomatic. It relies mainly on topical corticosteroids, oral antihistamines and oral cromolyn sodium therapy for gastrointestinal tract symptoms [2,3]. Education of parents to avoid precipitating factors is essential.
CONCLUSION
The diagnosis of UP can be made clinically but a definitive diagnosis requires a skin biopsy. In UP, systemic involvement is rare as in our patient and most childhood cases will experience a spontaneous resolution by adolescence.
CONSENT
The examination of the patient was conducted according to the Declaration of Helsinki principles. Written informed consent was obtained from the child’s parents for publication of this article.
REFERENCES
1. Dhar S, Maji B, Roy S, Dhar S. Diffuse Cutaneous Mastocytosis with Bullous Lesions and Pulmonary Involvement:A Rare Case. Indian J Dermatol. 2015;60:179-81.
2. Castells M, Metcalfe DD, Escribano L. Guidelines for the diagnosis and treatment of cutaneous mastocytosis in children. Am J Clin Dermatol. 2011;12:259-70.
3. Bajoghli AA, Blankenship CM. Picture of the month. Urticaria pigmentosa. Arch Pediatr Adolesc Med. 2008;162:383-4.
4. Macri A, Cook C. Urticaria Pigmentosa (Cutaneous Mastocytosis). Treasure Island (FL):Stat Pearls Publishing;2018.
5. Vasani RJ, Medhekar SV. Urticaria pigmentosa. Indian Dermatol Online J. 2015;6:464-5.
Notes
Source of Support: Nil
Comments are closed.