|
Get Citation
|
|
|
Gharaeinejad K, Rafiei R, Yousefkhani L, Rafiee B, Sheikhpour A. Simple congenital anonychia in an Iranian family. Our Dermatol |
|
|
Download citation file:
|
Simple congenital anonychia in an Iranian family
Kaveh Gharaeinejad1, Rana Rafiei2, Leila Yousefkhani1, Behnam Rafiee3, Abdolkarim Sheikhpour4
1Department of Dermatology, Skin Research Center, Guilan University of Medical Sciences, Razi Hospital, Sardare Jangal St. Rasht, Iran; 2Fellow Ship of Dermatopathology, Skin Research Center, Guilan University of Medical Sciences, Razi Hospital, Sardare Jangal St. Rasht, Iran; 3Research Internal, University of Texas, MD Anderson Cancer Center 1515 Holcombe blvd.B4.4512, Houston, USA; 4Medical Student, Guilan University of Medical Sciences, Razi Hospital, SardareJangal St. Rasht, Iran
Corresponding author: Rana Rafiei MD., E-mail: rafieirana@yahoo.com.
Submission: 07.08.2016; Acceptance: 25.10.2016
DOI: 10.7241/ourd.20172.50
ABSTRACT
Isolated congenital anonychia is a rare disorder which is presented by absence of fingernails and toenails since birth without other ectodermal and mesodermal abnormalities. Herein we present a 24-year-old man with anonychia in the hands and feet except in little toenails. Our patient had no abnormality in hair, teeth, skull, oral mucosa or intelligence. He was born from unaffected parents who were second degree relatives. He had no affected siblings but there were some affected persons in the second and third degree relatives so he was diagnosed as a simple autosomal recessive congenital anonychia.
Key words: Congenital; Simple anonychia; Autosomal recessive
INTRODUCTION
Nonsyndromic, isolated or simple anonycia is a rare entity which could be inherited by an autosomal dominant (AD) pattern with partial nail involvement or autosomal recessive (AR) pattern with severe nail involvement in an otherwise healthy person [1]. It is one of the rarest anomalies of the nails. Acquired anonychia and congenital syndromic anonychia which is associated with other abnormalities are more common than congenital nonsyndromic type [2].
CASE REPORT
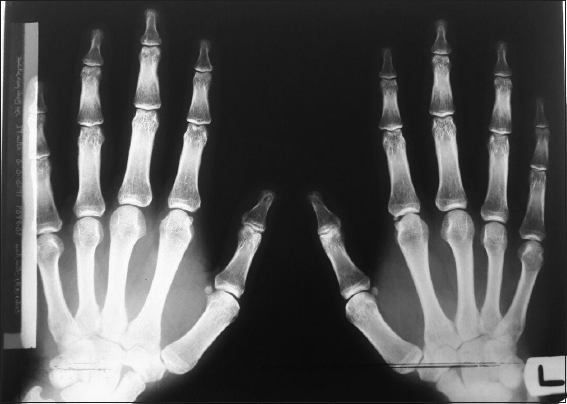
We report an Iranian 24-year-old man with anonychia (absence of nails) since birth. He had no finger nails and toenails except on the little toes. Nail folds, nail beds and distal phalanges were normal and the affected fingers were felt soft at their ends but he had no complaint of dysfunction (Figs. 1a and 1b). In physical examinations there were normal hairs, oral mucosa, tongue, teeth and head circumference. There was no icthyosis, palmoplantar keratoderma, skin pigmentation, dyshidrosis or mental retardation. For evaluation of ribs and distal phalanges radiographic imaging of the chest, hands and feet were done which revealed no abnormality (Fig. 2). He was born via normal vaginal delivery at term following an uncomplicated pregnancy without taking any medication.

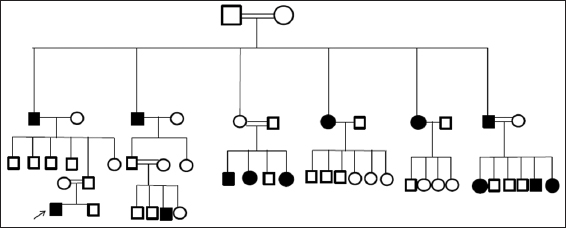
His parents and brother had normal nail plates but there were some affected persons in the second and third degree relatives which have been presented in the pedigree of the family (Fig. 3). This pedigree chart has been designed based on the information collected by our patient and we did not visit every single one, so information regarding other cousins and their children were not complete and our patient was not in touch with them anymore. Marriages in the families with affected children were consanguineous. These types of marriages are common in Iran especially in small towns.
DISCUSSION
Anonychia could be acquired or congenital. Common etiologies for acquired anonychia including trauma, pemphigus, lichen planus, epidermolysis bullosa and Stevens-Johnson syndrome [2,3].
Congenital anonychia could be syndromic, nonsyndromic or due to administration of a drug (phenytoin and warfarin) or viral infection during pregnancy [3,4]. Embriopathic nail diseases are hereditary but fetopathic disorders are nonhereditary and occur due to mechanical or vascular impairment in uterus [5].
Syndromic anonychia would be associated with other malformations including skeletal or neurological abnormalities, ectodermal dysplasia (dyshidrosis, skin pigmentation, hair and teeth abnormalities) and most of them would be inherited in an AD pattern. Nonsyndromic or simple anonychia is an isolated disorder without any other complications with an AD or AR inheritance pattern or sporadic mutation [3–5]. Both types of congenital anonychia could be presented by total or partial anonychia [4].
Our case was an AR nonsyndromic type of near total anonychia because he had unaffected parents, mixed sexes involvement in his pedigree of the family and history of multiple consanguineous marriages among second and third degree relatives. R-spondin gene mutation on chromosome 20 in exon 3 has been incriminated in AR simple anonychia [6]; also fragility on the long arm of the chromosome 10 has been reported [7]. Unfortunately we did not make genetic investigations for him due to lack of appropriate laboratory methods. We recommended his family to avoid consanguineous marriage to decrease incidence of disease.
In literature review there were rare case reports of total or near total simple anonychia with AR inheritance pattern especially in Iran, Saudi Arabia, Turkey, India and Kazakhstan probably due to consanguineous marriages [1–4,6,8–11]. We reported this case because of rare presentation but we guess it is not an extremely rare disorder and probably some of these cases have been unreported as it has been shown in our patient pedigree.
REFERENCES
1. Afsar FS, Karakuzu A. Total congenital anonychia. Pediatr Dermatol. 2014;31:743-4.
2. Yadalla HKK, Nitya R, Sujatha C. A rare case of isolated congenital complete simple anonychia. Int J Health Allied Scien. 2012;1:32-3.
3. Al Hawsawi K, Al Aboud K, Alfadley A, Al Aboud D. Anonychia congenita totalis: a case report and review of the literature. Int J Dermatol. 2002;4:397-9.
4. Rigopoulos D, Petropoulou H, Nikolopoulou M, Kalogirou O, Katsambas A. Total congenital anonychia in two children of the same family. J Eur Acad Dermatol Venereol. 2006;20:894-6.
5. Telfer NR, Barth JH, Dawber RPR. Congenital and hereditary nail dystrophies-an embryological approach to classification. Clinical and Experimental Dermatology. 1988;13:160-3.
6. Bruchle NO, Frank J, Frank V, Senderek J, Akar A, Koc E. RSPO4 is the major gene in autosomal-recessive anonychia and mutations cluster in the furin-like cysteine-rich domains of the Wnt signaling ligand R-spondin 4. J Inv Dermatol. 2008;128:791-6.
7. Ozyazgan I, Ozyazgan I, Dundar M. Isolated congenital anonychia cases with coincident chromosomal fragility. Ann Gen. 2004;47:381-6.
8. Mahloudji M, Amidi M. Simple anonychia. Further evidence for autosomal recessive inheritance. J Med Gen. 1971;8:478-9.
9. Qureshi A, Wong KY, Grant I. Congenital anonychia. J Hand Surg Eur. 2016;41:348-9.
10. Balta I, Kalkan G. A case report on autosomal recessive total congenital anonychia.Pediatr Dermatol. 2013;30:268-9.
11. Al Aboud K, Al Aboud D. Autosomal recessive total congenital anonychia in saudia family. Our Dermatol Online. 2013;4:496-7.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.