|
Get Citation
|
|
|
El Hadj OE, Bouhajja L, Goucha A, Hassouna JB, El May A, Gamoudi A. Calcifying fibrous tumor of axillary region. Our Dermatol Online. 2016;7(4):487-488. |
|
|
Download citation file:
|
Calcifying fibrous tumor of axillary region
Olfa El Amine El Hadj1, Leila Bouhajja1, Aida Goucha1, Jameleddine Ben Hassouna2, Ahmed El May1, Amor Gamoudi1
1Department of Pathology, Carcinological Institute Salah Azaiez, Tunis, Tunisia, 2Department of Carcinological Surgery, Carcinological Institute Salah Azaiez, Tunis, Tunisia
Sir,
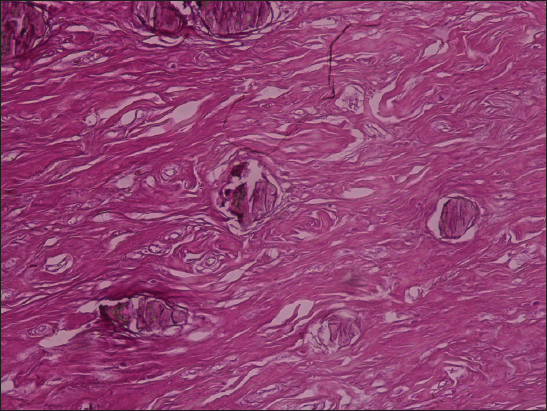
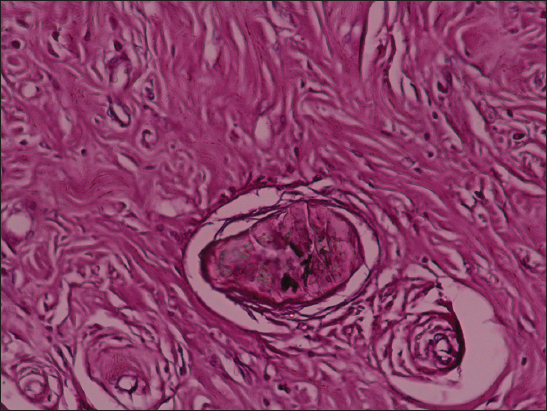
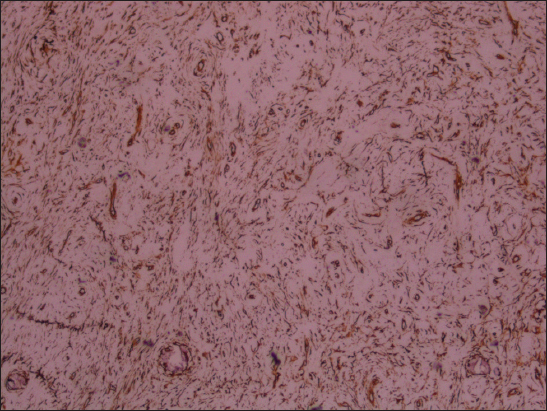
We report a 17 year-old woman who presented with a 1-year history of left axillary palpable mass. At physical examination the lesion was firm, lipomatous. The breast ultrasonography showed a left voluminous axillary mass, measuring 54mm, hyperechoic and ill limited. A surgical resection of the mass was performed. Grossly, it was a white firm well-circumscribed and lobed mass measuring 15x10x6 cm. Histological examination showed a benign mesenchymal tumor. It consisted of abundant fibrosis with hyalinised vessels, containing mononuclear infiltrate and foci of psammomatous calcifications (Fig. 1). Lymphoid follicles were noted around vessels and psammomas (Fig. 2). The tumor did not show any features of malignancy. Immunohistochemically, the spindle cells were vimentin positive (Fig. 3) and vessels showed CD34 positivity. These features confirmed the diagnosis of Calcifying fibrous tumors. At 4 years of follow-up, the patient was asymptomatic and there was no recurrence.

The patient’s informed consent was obtained.
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
Calcifying fibrous tumor (CFT) is a rare, usually solitary, benign tumor of uncertain etiology. The most common sites are the soft tissues of the extremities, pleura, or peritoneum [1]. It usually affects children and young adults, and it is composed of hyalinized fibrous tissue with dispersed bland fibroblastic spindled cells, scattered psammomatous, and/or dystrophic calcifications, and variably prominent mononuclear inflammatory infiltrate [2]. Macroscopically, CFT is well circumscribed and unencapsulated. Its diameter ranges from 1 to 15 cm. Their etiopathogenesis has not been fully clarified yet. However, in the literature, there are cases that may be related to trauma and Castleman’s disease [3]. Resection of CFT is usually curative. Local recurrence rate is approximately 10% [1].
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles. Written informed consent was obtained from the patient for publication of this article.
REFERENCES
1. Giardino AA, Ramaiya NH, Shinagare AB, Jagannathan JP, Stachler MD, Raut CP, Case report: Calcifying fibrous tumor presenting as an asymptomatic pelvic massIndian J Radiol Imaging 2011; 21: 306-8.
2. Jang KY, Park HS, Moon WS, Lee H, Kim CY, Calcifying fibrous tumor of the stomach: A case reportJ Korean Surg Soc 2012; 83: 56-9.
3. Gamsizkan M, Yildirim C, Daş K, Günhan Ö, Calcifying Fibrous Tumor: A Case ReportTurk Patoloji Derg 2015; 31: 141-4.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.