Dermatitis herpetiformis of Dhuring
Zoran Vrucinic, Dragana Starovic
Department of Dermatology, University Hospital Clinical Center, Banja Luka, Republic of Srpska, Bosnia and Herzegovina
How to cite this article: Vrucinic Z, Starovic D. Dermatitis herpetiformis of Dhuring. Our Dermatol Online. 2016;7(2):229
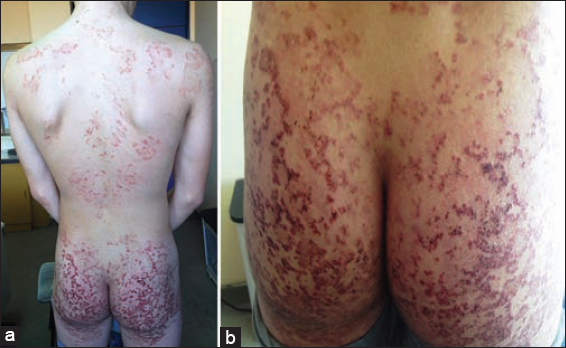
History: Presentation of 15th years old young man with first skin lesions started five years ago as erythematous rash on elbows and knees. After few months the lesions presented as confluent erythematous plaques on the skin of the extensor aspects of upper and lower extremities, back, neck and both gluteal regions (Figs. 1a and 1b). On the same places there are few single and linear excoriations and non adherent crusts with intense itching. From first skin lesions till nowadays, the patient was treated by several dermatologists under the diagnosis of pruritus, atopic dermatitis and eczematous dermatitis and used different types of local and systemic corticosteroids therapy, oral antibiotics antihistamines and one year of Dapsone 50mg a day, but without any therapeutic effects.
PHD analysis- (Irregular acanthosis of epidermis. Partially, signs of inter and intra fluid accumulation. Dermal papilla’s elongated and edematous. In single papilla’s are groups of neutrophilic granulocytes (microabscess). Focal, in papilla’s, presens of small splits filled with fibrin and neutrophilic granulocytes. Capillary blood vessels of the upper dermis are dilated, lined with hyperplastic and hypertrophic endothelial cells. Around are lymphocytic and neutrophilic granulocytes (PHD No 508/03.12.2014. confirmed the diagnosis of Dermatitis Herpetiformis)
Laboratory Examinations: Tranglutamine Antibody IgA 113 U/ml (lower limit 10 U/ml), Transglutamine Antibody IgG negative. (05.12.2015)
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.