Primary squamous cell carcinoma kidney: A rare case report
Vijay Domblae, Shivanand Gundalli, MH Prabhu, Singhania Somil, Sonali
Department of Pathology, S N Medical College, Bagalkot, Karnataka, India
ABSTRACT
Primary squamous cell carcinoma (SCC) of the kidney is a very rare clinical entity. Only a few cases have been reported in world literature. Here we report a case with renal SCC. The patient presented with flank pain, fever and vomiting. In ultrasonography, renal mass was detected and after nephrectomy followed by histopathological examination, it was diagnosed as SCC. It was associated with renal calculi and hydronephrosis. The lack of characteristic presentation like hematuria, pain and palpable mass causes delay in diagnosis results in locally advanced or metastatic disease at presentation.
Key words: Renal; Carcinoma; Squamous cell carcinoma
INTRODUCTION
Primary neoplasms of the renal collecting system are uncommon accounting for only 4% to 5% of all urothelial tumours. The transitional cell type is the most frequently diagnosed (85%-95%) followed by squamous cell carcinoma (6%-15%) [1]. Squamous cell carcinoma of the renal pelvis is a rare tumour. The incidence of this tumour is 1.4% of all renal malignancy [2]. Primary renal squamous cell carcinoma is a very rare tumour and few cases have been reported in world literature [3].
CASE REPORT
A 68 year old female patient presented with complaints of pain in the right flank pain for 2 month. Fever and chills for 15 days. Physical examination was unremarkable Routine haematology revealed. neutrophilic leucocytosis and moderate degree of normochromic normocytic anemia. Ultrasonography of abdomen and CT showed enlarged right kidney with loss of normal renal architecture and a large mass measuring (5×4.) cm. On gross examination, the kidney was larger in size measuring (11×5) cm.
Cut surface revealed (Fig. 1) Variegated G/W solid areas, thinned out cortex, dilated calyces and a large stone. Growth of tumour was infiltrating in nature.

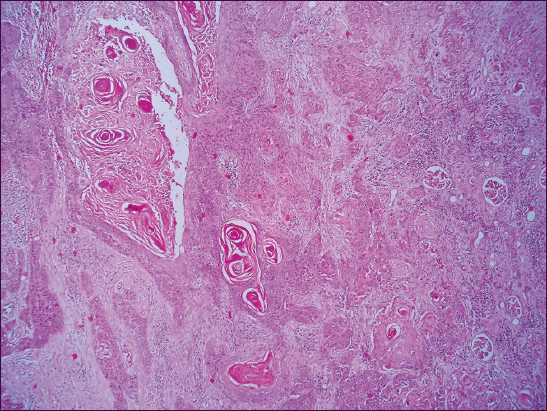
Histopathological examination revealed features of Well differentiated invasive squamous cell carcinoma with urolithiasis (Fig. 2).
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Squamous cell carcinoma of the renal collecting system is a rare malignancy with poor prognosis accounting for about 10 % of renal pelvic tumors and 0.5 % of all renal tumors [4,5]. They are frequently associated with long standing staghorn calculi, chronic kidney infection, hydronephrosis and analgesic abuse [5]. Hypercalcemia, leukocytosis and trombocytosis have been reported as a part of paraneoplastic syndromes in RSCC cases [6,7]. Although being nonspecific, a solid mass, hydronephrosis and calcifications are common radiologic findings, which may explain why the diagnosis could be missed before the histopatological examination.
In a series of 4 patients with squamous cell carcinoma of renal pelvis, mean age was 60 yrs. M: F was 3:1, right to left side ratio was 1:1 and most common presenting symptom was flank pain and haematuria. In 100% of cases, there was presence of staghorn type of renal stones [8].
Renal pelvic tumours are almost never palpable clinically, however they may block the urinary out flow and lead to palpable hydronephrosis.
Hydronephrosis is more common in renal tumour than renal pelvic ones2. In 50% of renal pelvic tumours there is precxisting or concomitant bladder urothelial tumour [9].
In general, these tumours are highly aggressive and are at high stage when detected. Most of them are histologically high grade and outcome is generally unfavorable. Extensive infiltration of the renal parenchyma and retroperitoneal soft tissues are very common [10]. In one series, 84% of the tumour were found at operation to be locally advanced or metastatic [11]. The prognosis was very poor. The current primary treatment of renal squamous cell carcinoma is nephrectomy with or without ureterectomy3 followed by radiotherapy and chemotherapy.
In the present case the patient was 68 yrs old, presented with flank pain, fever and chills. Associated etiological factors like Calculi and hydronephrosis were detected.
Grossly, infiltrative pattern of tumour mass occupied most of the renal parenchyma was seen. So the origin of the tumour was from renal parenchyma not from renal pelvis.
CONCLUSION
Squamous cell carcinoma of urothelial tract particularly renal pelvis is thought to arise through a process of metaplasia of urothelium. Various etiological factors are responsible for squamous metaplasia and subsequent carcinoma.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles
REFERENCES
1. Karabulut A, Emir L, Gonultas M, Incel N, Germiyanoglu C, Squamous cell carcinoma located in the renal calyceal system;A case report and review of the literatureTurk J Cancer 2002; 32: 20-4.
2. Bandyopadhyoy R, Biswas S, Nag D, Ghosh AK, Squamous cell carcinoma of the renal pelvis presenting as hydronephrosisJ Can Res Ther 2010; 6: 537-9.
3. Singh V, Sinha RJ, Sankhwar SN, Mehrotra B, Ahmed N, Squamous cell carcinoma of the kidney-rarity redefined;Case series with review of literatureJ Cancer Sci Ther 2010; 2: 55-6.
4. Blacher EJ, Johnson DE, Abdul-Karim FW, Ayala AG, Squamous cell carcinoma of renal pelvisUrology 1985; 25: 124-6.
5. Busby JE, Brown GA, Tamboli P, Kamat AM, Dinney CP, Grossman HB, Upper urinary tract tumors with nontransitional histology: a single-center experienceUrology 2006; 67: 518-23.
6. Cadeddu JA, Jarrett TW, Hypercalcemia associated with squamous cell carcinoma of the renal pelvisJ Urol 1998; 160: 1798.
7. Er O, Coskun HS, Altinbas M, Akgün H, Cetin M, Eser B, Rapidly relapsing squamous cell carcinoma of the renal pelvis associated with paraneoplastic syndromes of leukocytosis, thrombocytosis and hypercalcemiaUrol Int 2001; 67: 175-7.
8. Jain A, Mittal D, Jindal A, Solanki R, Khatri S, Parikh A, Incidentally detected squamous cell carcinoma of renal pelvis in patients with staghorn calculi; case series with review of the literatureISRN Oncol 2011; 2011: 620574.
9. Al Pers CE, Kumar V, Abbus AK, Fausto N, Aster J.C, The kidney inPathologic basis of disease 8th ed. Philadedphila, USA: Saunders; 967-2010.
10. Fletcher CDM, Tumours of the urinary tract; Diagnostic Histopathology of tumours 2007; 3rd ed. Philadelphia: Elsevier; 522-523.
11. Rosai J, Urinary tract, surgical pathology Vol I: 9th ed. st louis USA: MOSBY; 1274-2004.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.