Nevoid acanthosis nigricans: a rare case with late onset
Mrinal Gupta1, Vikram K Mahajan1, Suman Singh2
1Department of Dermatology, Venereology & Leprosy, Dr. R. P. Govt. Medical College, Kangra (Tanda) -176001 (Himachal Pradesh), India,2Department of Pathology, Dr. R. P. Govt. Medical College, Kangra (Tanda) -176001 (Himachal Pradesh), India
ABSTRACT
Nevoid acanthosis nigricans is a rare variant usually presents as a localized hyperpigmented velvety plaque at birth or before puberty. However, unlike other variants, it is neither localized to the neck or flexures nor associated with metabolic disturbances, syndromes, drug toxicity, endocrinopathy or malignancy. Only a few cases of nevoid acanthosis nigricans have been reported in the literature. This 17-year-old male presented with a gradually progressive hyperpigmented, velvety plaque of nevoid acanthosis nigricans over the midline of the abdomen having a late onset.
Key words: Nevoid acanthosis nigricans; Acanthosis nigricans; Epidermal nevus
INTRODUCTION
Acanthosis nigricans is a disorder of keratinization classically characterized by hyperpigmented velvety plaques localized mainly over neck, axillae and the inguinal folds. Depending upon the underlying systemic abnormality it has been classified as obesity-associated, benign, syndromic, malignant, acral, unilateral, drug-induced and mixed-type acanthosis nigricans. The nevoid acanthosis nigricans is a rare form which presents at birth or before puberty as a solitary well-defined hyperpigmented velvety plaque, usually localized to body areas other than those involved by classic AN and is not associated with any underlying disorder [1]. The described case is of classic nevoid acanthosis nigricans localized over the abdomen with a late onset.
CASE REPORT
A 17-year-old boy presented with a gradually progressive, asymptomatic, hyperpigmented plaque over the midline of abdomen for three months. The lesion had begun as a small hyperpigmented plaque initially over the epigastrium that gradually increased in size and progressed to reach the mid abdomen. The patient was a second child of non-consanguineous parentage and had no family history of similar lesion. He was not obese (BMI 21.4) and had no past or concurrent history of diabetes mellitus, drug intake or other associated systemic complaints. Clinical examination showed a well-defined hyperpigmented, velvety plaque with irregular margins, measuring 12 × 5 cm over abdomen extending between epigastrium and supra umbilical area with predominant left-to-midline localization (Fig. 1). There were no other lesions of similar morphology present over neck or the flexural folds. A few acneiform lesions were noted over chest. Examination for hair, nails, mucous membranes and other systems was unremarkable. Laboratory investigations including blood counts, blood glucose levels, hepato-renal function tests, thyroid function tests, growth hormone assays and urinalysis were normal. X-rays for chest, skull and long bones, and abdominal ultrasonography revealed no abnormality. A skin biopsy from the lesion revealed hyperkeratosis, papillomatosis and mild acanthosis in the epidermis (Fig. 2). There was mild mixed inflammatory infiltrate in the upper dermis. In view of these clinicopathologic features, a diagnosis of nevoid acanthosis nigricans was made. He was prescribed topical 0.05% tretinoin gel for once daily application. The lesional thickness and pigmentation decreased to some extent after 2 months of therapy. He did not turn up further.
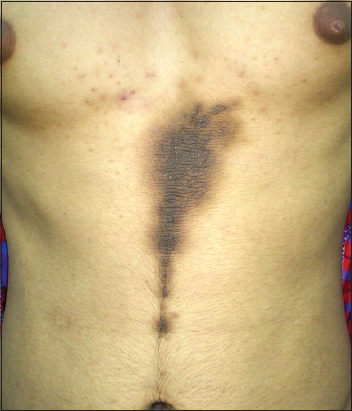
Figure 1: A well-defined hyperpigmented, velvety, plaque of typical nevoid acanthosis nigricans over abdomen extending between epigastrium and supra umbilical area with predominant left-to-midline localization.
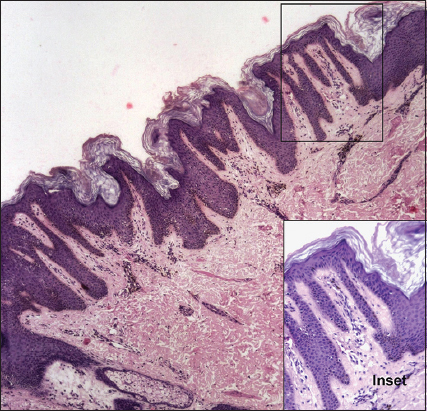
Figure 2: Epidermis shows mild hyperkeratosis with basket weave appearance, mild acanthosis, elongated rete ridges and prominent papillomatosis with minimal inflammatory cell infiltrate in papillary and upper dermis, (H&E, ×10, Inset ×40).
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Nevoid acanthosis nigricans is a rare dermatosis usually presenting as a solitary, localized lesion over body. It may present at birth, during childhood or appear at puberty. The exact underlying pathomechanism in the development of nevoid acanthosis nigricans remains speculative. It has been postulated to be inherited irregularly as an autosomal dominant trait and the mosaic expression of activated growth factor receptors in keratinocytes has been hypothesized to play a role in its pathogenesis [1–3]. Clinically, it appears as a well-defined hyperpigmented, velvety plaque resembling classic acanthosis nigricans without any flexural predisposition while chest, abdomen, umbilicus, retroauricular area and the submammary area being the predominant sites of involvement in most cases [1–5]. Occasionally it presents along the lines of Blaschko. It may enlarge initially but tends to remain stable or may even regress over time. The closest differential diagnosis is epidermal nevus but acanthosis nigricans lesions are usually more velvety and histologically show mild compact hyperkeratosis, papillomatosis, and limited acanthosis as compared to epidermal nevi. The affected individuals often seek treatment for cosmetic reasons. However, no therapeutic recommendations exist. Some workers have noted efficacy of topical tretinoin that largely remains unevaluated for paucity of cases [1,5]. This patient exhibited more or less similar clinical and histologic features of typical nevoid acanthosis nigricans exhibiting partial improvement with topical tretinoin before he stopped follow up.
CONSENT
The examination of the patient was conducted according to the Declaration of Helsinki principles. Written informed consent was obtained from the patient for publication of this article.
REFERENCES
1. Jeong JS, Lee JY, Yoon TY, Unilateral nevoid acanthosis nigricans with a submammary locationAnn Dermatol 2011; 23: 95-7.
2. Colegio OR, McNiff JM, Antaya RJ, Nevoid acanthosis nigricans with subtle melanocyte hyperplasiaJ Am Acad Dermatol 2008; 58: 5 Suppl 1102-3.
3. Das JK, Sengupta S, Gangopadhyay A, Nevoid acanthosis nigricansIndian J Dermatol Venereol Leprol 2008; 74: 279-80.
4. Kim SK, Kim YC, Nevoid acanthosis nigricans localized to the umbilicusJ Dermatol 2006; 33: 433-4.
5. Lee JH, Kim MY, Kim HO, Park YM, Nevoid acanthosis nigricans localized to the umbilicus: successful treatment with topical tretinoinAnn Dermatol 2005; 17: 24-6.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.