Our Dermatol Online. 2012; 3(1): 36-42
Date of submission: 08.10.2011 / acceptance: 08.12.2011
Conflicts of interest: None
IMMUNOFLUORESCENCE IN MULTIPLE TISSUES UTILIZING SERUM FROM A PATIENT AFFECTED BY SYSTEMIC LUPUS ERYTHEMATOSUS
Ana Maria Abreu Velez1, Michael S. Howard1, Piotr Brzezinski2
1Georgia Dermatopathology Associates, Atlanta, Georgia, USA
2Dermatological Clinic, 6th Military Support Unit, Ustka, Poland
Corresponding author: Ana Maria Abreu-Velez, MD PhD e-mail: abreuvelez@yahoo.com
How to cite an article: Abreu Velez AM, Howard MS, Brzezinski P. Immunofluorescence in multiple tissues utilizing serum from a patient affected by systemic lupus erythematosus. Our Dermatol Online 2012; 3(1): 36-42.
Abstract
Introduction: Lupus erythematosus is a chronic, inflammatory autoimmune disease that can affect multiple organs. Lupus can affect many parts of the body, especially in systemic lupus erythematosus (SLE); affected tissues may include the joints, skin, kidneys, heart, lungs, blood vessels, and brain. Case report: A 46-year-old female presented with pruritus, photosensitivity and edema of the cheeks of about 2 years duration, and was evaluated by a dermatologist. On examination, multiple telangiectasias were present on the cheeks, with erythema, edema and a malar rash observed. A review of systems documented breathing difficulty and pleuitic pain, joint pain and joint edema, photosensitivity, cardiac dysrhythmia, and periodic pain in the back close to the kidneys. Methods: Skin biopsies for hematoxylin and eosin testing, as well for direct and indirect immunofluorescence were performed, in addition to multiple diagnostic blood tests, chest radiography and directed immunologic testing. Results: The blood testing showed elevated C-reactive protein. Direct and indirect immunofluorescence testing utilizing monkey esophagus, mouse and pig heart and kidney, normal human eyelid skin and veal brain demonstrated strong reactivity to several components of smooth muscle, nerves, blood vessels, skin basement membrane zone and sweat gland ducts and skin meibomian glands. Anti-endomysium antibodies were detected as well as others, especially using FITC conjugated Complement/C1q, FITC conjugated anti-human immunoglobulin IgG and FITC conjugated anti-human fibrinogen. Conclusions: We conclude that both direct and indirect immunofluorescence using several substrates can unveil previously undocumented autoantibodies in multiple organs in lupus erythematosus, and that these findings could be utilized to complement existing diagnostic testing for this disorder.
Key words: Systemic lupus erythematosus; smooth muscle antibodies; monkey esophagus; direct and indirect immunofluorescence; autoantibodies
Abbreviations:
Systemic lupus erythematosus (SLE), antinuclear antibodies (ANA), subacute cutaneous LE (SCLE), basement membrane zone (BMZ), chronic discoid LE (DLE), direct immunofluorescence (DIF), indirect immunofluorescence (IIF), 4′,6-diamidino-2-phenylindole (DAPI), American College of Rheumatology Criteria (ACRC)
Introduction
Systemic lupus erythematosus (SLE) is a chronic, potentially fatal autoimmune disease characterized by immune dysregulation; the dysregulation results in the production of antinuclear antibodies (ANAs), generation of circulating immune complexes, and activation of the complement system. The disease often manifests unpredictable exacerbations and remissions, and unpredictable clinical manifestations [1-5]. In SLE, there is an elevated probability for clinical involvement of the joints, kidney, brain, lung, heart, serosa and gastrointestinal tract [1-5]. Women and minorities are disproportionately affected; SLE is most common in women of child-bearing age, although it has been reported in extremes of life (e.g., in infants and through the tenth decade of life) [1-5]. The prevalence of lupus erythematosus in the United States has been estimated from approximately 250,000 patients to as high as 2,000,000. The pathologic hallmark of the disease is recurrent, widespread, and diverse vascular lesions [1-5]. In the 60% of SLE patients who experience the onset of their disease between puberty and the fourth decade of life, the female to male ratio is 9:1. Lupus is three times more frequent in African Americans than in American Caucasians [1-5]. The ethnic group at greatest risk is African Caribbean blacks. The annual incidence of SLE ranges from six to 30 new cases per 100,000 population in relatively low-risk to high-risk groups [1- 5]. The American College of Rheumatology Criteria (ACRC) for lupus erythematosus were developed to nosologically define patients with this disorder [6]. The ACRC represent 11 criteria to establish a diagnosis of this disease. A patient must present four or more of the criteria to be classified as having lupus. These criteria are also utilized to insure the appropriateness of subjects for epidemiological or research studies. Although many patients do not fulfill the diagnostic criteria at first encounter, many do so when followed over time [6].
Case Report
A 46 year old female visited the dermatologist for a two year history of skin tightening with pruritis and marked light hypersensitivity, especially on the skin of the face. On examination, erythematous, edematous areas were present on the cheeks, with multiple telangiectasis also noted. The patient’s C-reactive protein value was 21.3 mg/l (normal limits to 4.0 mg/l); her white blood cell count (WBC) at 9.6 x10^3ul (4.0-10 x10^3ul normal value), with basophils at 0.5% (0.1-1.6% normal value), eosinophils at 0.7% (0,1-0.6% normal value), neutrophils at 6.6% (2.9-6.2% normal value), lymphocytes at 1.6% (1.8-8.4% normal values), and monocytes at 0.5% (0.15- 1.3% normal value). Thyroid testing values were within normal limits. Other laboratory tests, including total peripheral blood protein, albumin, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, and total and direct bilirubin were within normal limits. Antinuclear antibodies (ANA) were positive, at 1:160 with a homogeneous pattern (up to 1:80 normal value). Anti-cyclic citrullinated peptide antibodies (aCCP) were present at 9 EliA U/ml(normal limits: 7-10 EliA U/ml), and after 1 month increased to 10 EliA U/ml. No oral ulcers or neurological disorders were documented. Anti- DNA antibodies were negative; a Venereal Disease Research Laboratory test (VDRL) was also negative, and kidney function was normal. On physical exam, a sensitive area was present on the back in the area of the kidneys. The EKG demonstrated showed some cardiac dysrhythmia. The patient also related periodic chest pain, and pleuritic pain was detected on examination. Other physical examination findings included knee and elbow pain, edema and erythema; small cysts of the left ulna and of the ossa metacarpi were also detected. A thickening of the pleura on one right lung lobe was observed by chest radiography. Following workup, the patient was diagnosed with systemic lupus erythematosus (SLE), and prednisone (5mg per day) was prescribed for 2 months plus Niacin™ (200mg daily) and Rantydyne™ (300mg daily). Following this treatment, the patient did not show skin lesion improvement. Thus, these medications were discontinued and topical tacrolimus and metronidazole cream was initiated on the facial lesions.
Materials and Methods
A punch biopsy of the skin was performed for hematoxylin and eosin (H&E) analysis, as well as for multicolor direct and indirect immunofluorescence (DIF, IIF) utilizing multiple antigen tissues as substrates including monkey esophagus, porcine and murine heart and kidney, human eyelid and others. The tests were performed ultilizing previously described techniques and antibodies [7-13].
Results
Hematoxylin and Eosin staining
H&E staining displayed histologic features of a mild interface dermatitis, including hydropic degeneration of the basal cell layer. An associated superficial, perivascular dermal infiltrate of lymphocytes and histiocytes was present; upper dermal edema and perivascular extravasation of erythrocytes was also observed. The H&E, DIF and IIF results are summarized in the Figures 1-3.
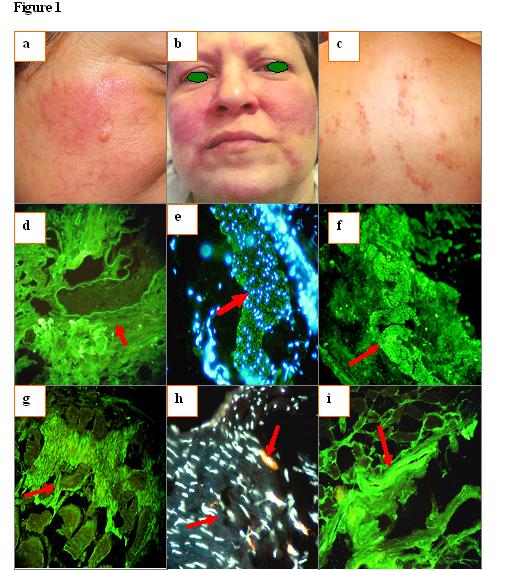 Figure 1. a through c, clinical pictures demonstrating erythematous, edematous plaques on the cheeks with fine telangiectasias. d. DIF demonstrating linear FITC conjugated Complement/C3 deposits along the BMZ of the hair follicle (yellow staining; red arrow). e. IIF on monkey esophagus substrate, demonstrating positive staining of the endomysium utilizing FITC conjugated anti-human Complement/C1q(green staining; red arrow); the nuclei of the substrate cells are counterstained in blue using DAPI. f. Similar to e, but without nuclear counterstaining. g. IIF on monkey esophagus substrate, demonstrating positive staining against smooth muscle utilizing FITC conjugated anti-human Complement/C1Qq(green staining; red arrow). h. IIF on monkey esophagus substrate, demonstrating positiviy against small blood vessels utilizing Alexa Fluor 647 conjugated anti-human IgG(orange staining; red arrows). i. IIF on monkey esophagus substrate, demonstrating positivity against larger blood vessels utilizing FITC conjugated anti-human fibrinogen (green staining; red arrow)
|
 Figure 2. a. IIF on monkey esophagus substrate, demonstrating positivity against a large nerve utilizing FITC conjugated anti-human Complement/C1q(green staining; red arrows). b. IIF on monkey esophagus substrate, demonstrating positivity against several smooth muscle bundles utilizing FITC conjugated anti-human albumin (green staining; red arrows). Muscle cell nuclei are counterstained with DAPI in blue. c. IIF on monkey esophagus substrate, demonstrating linear positivity against the BMZ (light green staining; red arrow) using FITC conjugated anti-human Complement/C1q FITC and against the endomysium (white arrow). d. IIF on monkey esophagus substrate, displaying positivity against the internal layer of the esophagus resembling a pattern of anti-fibrillagrin antibodies, using FITC conjugated anti-human Complement/C3 (green staining; red arrows). The nuclei of the cells are counterstained with DAPI(blue staining). e. DIF of skin demonstrating positivity against an eccrine sweat gland ductus using FITC conjugated anti-human IgG (red arrow), against the BMZ (white arrow), and some intercellular staining in some patches of the epidermal stratum spinosum (blue arrow). Finally, note the orange staining against small blood vessels using Alexa Fluor 647 conjugated anti-human IgG(yellow arrows). f. Similar to e, but in this case we counterstained the nuclei with Dapi (blue staining). The white arrow shows reactivity against the acrosyringium, the yellow arrows against the blood vessels and the red arrow against a sweat gland ductus
|
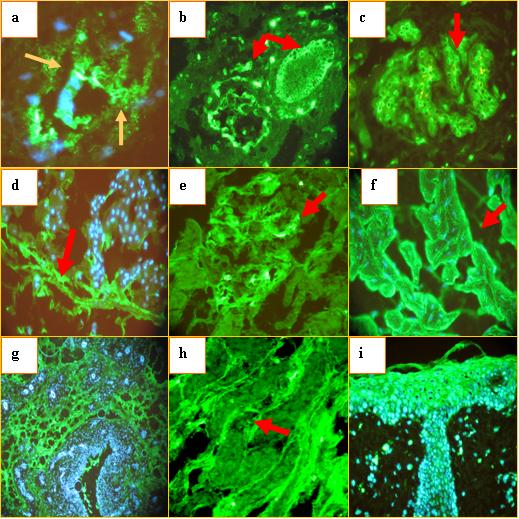 Figure 3. a. IIF utilizing veal brain shows immunoreactivity to several vessels using FITC conjugated anti-human fibrinogen (green staining, yellow arrows). The nuclei were counterstained with DAPI(blue). b. IIF utilizing normal human skin from an eyelid cosmetic surgery, and utilizing FITC conjugated anti-human Complement/C1q antibodies directed against the meibomian glands and their ducts (green staining, red arrows). c. Same tissue and antibody as in b; in this case, the antibodies recognized the modified sweat glands of the eyelids(green staining; red arrow). d. IIF utilizing murine kidney shows immunoreactivity to the capsule of the kidney using FITC conjugated anti-human fibrinogen(green staining; red arrow). The nuclei were counterstained with DAPI(blue). e. Similar to d, but in this case the positivity is against renal glomeruli(green staining; red arrow). f. IIF using porcine heart demonstrates immunoreactivity to several cardiomyocytes using FITC conjugated anti-human-IgG FITC(green staining, red arrow). The nuclei were again counterstained with DAPI in blue. g. IIF utilizing porcine instestine demonstrates immunoreactivity to several cells using FITC conjugated antihuman-IgG FITC(green staining, red arrow). The nuclei were counterstained with DAPI. h. IIF using murine kidney shows immunoreactivity to a kidney tubule utilizing FITC conjugated anti-human fibrinogen(green staining, red arrow). i. IIF utilizing normal human eyelid skin from cosmetic surgery using FITC conjugated anti-human Complement/C1q antibodies directed against epidermal keratinocytes in a perinuclear fashion (green staining). Keratinocyte nuclei are counterstained in blue with DAPI
|
Discussion
The precise etiology of SLE remains unidentified. A genetic predisposition, sex hormones, and environmental trigger(s) likely result in the dysregulated immune response that typifies the disease [1-5]. A role for genetics and environmental factors is suggested by the increased incidence of the disease in selected families and geographic regions [1-5]. A clinical cutaneous presentation of lupus erythematosus might include some SLE findings with findings of other variants, such as chronic discoid or subacute cutaneous lupus. However, the most common skin lesions seen in SLE are those of the acute type (including a malar rash with photosensitivity and telangiectasias), as demonstrated in this case [14-19]. DIF and IIF studies on skin samples for lupus have classically shown granular and/or linear deposits of IgG, IgA and IgM along the basement membrane zone of the skin, and selected immunoreactants present surrounding dermal blood vessels [14-18]. However, deposits of immunoglobulins and complement have been also recently documented to dermal sweat glands, sebaceous glands and nerves [7,8,10-12]. (TU OBRAZEK) Figure 3. a. IIF utilizing veal brain shows immunoreactivity to several vessels using FITC conjugated anti-human fibrinogen (green staining, yellow arrows). The nuclei were counterstained with DAPI(blue). b. IIF utilizing normal human skin from an eyelid cosmetic surgery, and utilizing FITC conjugated anti-human Complement/C1q antibodies directed against the meibomian glands and their ducts (green staining, red arrows). c. Same tissue and antibody as in b; in this case, the antibodies recognized the modified sweat glands of the eyelids(green staining; red arrow). d. IIF utilizing murine kidney shows immunoreactivity to the capsule of the kidney using FITC conjugated anti-human fibrinogen(green staining; red arrow). The nuclei were counterstained with DAPI(blue). e. Similar to d, but in this case the positivity is against renal glomeruli(green staining; red arrow). f. IIF using porcine heart demonstrates immunoreactivity to several cardiomyocytes using FITC conjugated anti-human-IgG FITC(green staining, red arrow). The nuclei were again counterstained with DAPI in blue. g. IIF utilizing porcine instestine demonstrates immunoreactivity to several cells using FITC conjugated antihuman- IgG FITC(green staining, red arrow). The nuclei were counterstained with DAPI. h. IIF using murine kidney shows immunoreactivity to a kidney tubule utilizing FITC conjugated anti-human fibrinogen(green staining, red arrow). i. IIF utilizing normal human eyelid skin from cosmetic surgery using FITC conjugated anti-human Complement/C1q antibodies directed against epidermal keratinocytes in a perinuclear fashion (green staining). Keratinocyte nuclei are counterstained in blue with DAPI The origin of autoantibody production in SLE is uncertain; suggested possibilities have included an antigen driven process, spontaneous B-cell hyperresponsiveness, or impaired immune regulation. Regardless of the etiology of autoantibody production, SLE is associated with impaired clearance of circulating immune complexes [1-5]. More is known about the pathogenic cellular and molecular events which are responsible for the vascular lesions in SLE than regarding the precise origins of the autoimmunity [1-5]. Disease manifestations result from recurrent vascular injury due to immune complex deposition, leukothrombosis, or thrombosis [1-5]. Additionally, cytotoxic antibodies can mediate autoimmune hemolytic anemia and thrombocytopenia, while antibodies to specific cellular antigens can disrupt cellular function. An example of the latter is the association between antineuronal antibodies and neuropsychiatric SLE [1-5]. In our study, our DIF and IIF results and the patient review of the systems directed us to search for damage in other organs, especially antibodies to smooth muscle and blood vessels. This patient was found to have pleuritis; some authors have also described pleuitic antibodies to be present in cases of SLE [20,21]. Our findings are of interest, because tests other than classical antibody testing may be of value in the diagnosis of SLE. Recently, murine liver and kidney, and epithelial cell lines obtained from human laryngeal carcinoma (including Hep-2) have been explored as substrates for ANA testing. Such ANA testing has high diagnostic sensitivity, and most ANAs are of IgG isotype [23]. Other autoantibodies routinely tested for lupus and anti-cytoplasmic antibodies (such as anti-Ro/SSA and anti–t-RNA synthetases) are not always readily detected on these substrates due to scarcity of the antigen in Hep- 2 cells, and/or antigen leaching and denaturation secondary to fixation procedures [23]. At present, of the approximately 40 types of possible diagnostic fluoroscopic patterns identified in one pertinent study, only 19 are directly associated with clinical diagnoses; moreover, for many autoantibodies, the target autoantigen has not been identified with certainty [23]. We thus conclude that there are several patterns of autoantibodies that have not been well elucidated, and could assist in the laboratory diagnosis of SLE.
Conclusion
We present the case for the unusual clinical presentation in an adult patient (bulky lesions showed a rare anatomical site), having to resort to auxiliary diagnostic methods, and the satisfactory therapeutic response.
REFERENCES
1. Hochberg MC: Systemic lupus erythematosus. Rheum Dis Clin North Am. 1990; 16: 617-639. 2. Arnold HL Jr: Systemic lupus erythematosus.AMA Arch Derm Syphilol. 1950; 62: 632-634. 3. Aringer M, Hiepe F: Systemic lupus erythematosus.Z Rheumatol. 2011; 70: 313-323. 4. Chang C, Gershwin ME: Drug-induced lupus erythematosus: incidence, management and prevention.Drug Saf. 2011; 34: 357-374. 5. Tebbe B, Mansmann U, Wollina U, Auer-Grumbach P, Licht-Mbalyohere A, Arensmeier M, Orfanos CE: Markers in cutaneous lupus erythematosus indicating systemic involvement. A multicenter study on 296 patients. Acta Derm Venereol. 1997; 77: 305-308. 6. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al: The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982; 25: 1271-1277. 7. Abreu-Velez AM, Smith JG Jr, Howard MS: Activation of the signaling cascade in response to T lymphocyte receptor stimulation and prostanoids in a case of cutaneous lupus. North Am J Med Sci. 2011; 3: 251-254. 8. Abreu Velez AM, Smith JG Jr, Howard MS: Cutaneous lupus erythematosus with autoantibodies colocalizing with glial fibrillary acidic protein. N Dermatol Online. 2011; 2: 8-11. 9. Howard MS, Yepes MM, Maldonado JG, Villa E, Jaramillo A, Botero J, et al: Broad histopathologic patterns of non-glabrous skin and glabrous skin from patients with a new variant of endemic pemphigus foliaceus (part 1). J Cutan Pathol. 2010; 37: 222-230. 10. Abreu Velez AM, Smith JG Jr, Howard MS: Vimentin compartamentalization in discoid lupus. North Am J Med Sci. 2010; 2: 106-110. 11. Abreu Velez AM, Howard MS, Loebl AM: Autoreactivity to sweat and sebaceous glands and skin homing T cells in lupus profundus. Clin Immunol. 2009; 132: 420-424. 12. Abreu Velez AM, Girard JG, Howard MS J: Antigen presenting cells in a patient with hair loss of and systemic lupus erythematosus. North Am J Med Sci. 2009; 1: 205-210. 13. Abreu Velez AM, Smith JG Jr, Howard MS: Neutrophil extracellular traps (NETS), IgD, myeloperoxidase (MPO) and antineutrophil cytoplasmic antibody (ANCA) associated vasculitides. North Am J Med Sci. 2009; 1: 309-313. 14. Watanabe T, Tsuchida T: Classification of lupus erythematosus based upon cutaneous manifestations. Dermatological, systemic and laboratory findings in 191 patients. Dermatology. 1995; 190: 277-283. 15. Grönhagen CM, Fored CM, Granath F, Nyberg F: Cutaneous lupus erythematosus and the association with systemic lupus erythematosus: a population-based cohort of 1088 patients in Sweden. Br J Dermatol. 2011; 164: 1335-1341. 16. Tebbe B: Clinical course and prognosis of cutaneous lupus erythematosus. Clin Dermatol. 2004; 22: 121-124. 17. Cardinali C, Caproni M, Bernacchi E, Amato L, Fabbri P: The spectrum of cutaneous manifestations in lupus erythematosus–the Italian experience.Lupus. 2000; 9: 417-423. 18. Vera-Recabarren MA, García-Carrasco M, Ramos- Casals M, Herrero C: Comparative analysis of subacute cutaneous lupus erythematosus and chronic cutaneous lupus erythematosus: clinical and immunological study of 270 patients. Br J Dermatol. 2010; 162: 91-101. 19. Kuhn A, Schuppe HC, Ruzicka T, Lehman P: Rare cutaneous manifestations of lupus erythematosus. A clinical overview. Hautarzt. 2000; 51: 818-825. 20. Velthuis PJ, Kater L, van der Tweel I, de la Faille HB, van Vloten WA: Immunofluorescence microscopy of healthy skin from patients with systemic lupus erythematosus: more than just the lupus band. Ann Rheum Dis. 1992; 51: 720–725. 21. Guo H, Leung JC, Chan LY, Chan TM, Lai KN: The pathogenetic role of immunoglobulin G from patients with systemic lupus erythematosus in the development of lupus pleuritis. Rheumatology (Oxford). 2004; 43: 286- 293. 22. Ngian GS, Naidoo P, Morand EF, Hoi AY: Smooth muscle myopathy as an underrecognized manifestation of active systemic lupus erythematosus. Intern Med J. 2011; 41: 495-498. 23. Tozzoli R, Bizzaro N, Tonutti E, Villalta D, Bassetti D, Manoni F, et al: Italian Society of Laboratory Medicine Study Group on the Diagnosis of Autoimmune Diseases. Guidelines for the laboratory use of autoantibody tests in the diagnosis and monitoring of autoimmune rheumatic diseases. Am J Clin Pathol. 2002; 117: 316-324.
Comments are closed.