Our Dermatol Online. 2012; 3(1): 21-23
Date of submission: 04.08.2011 / acceptance: 19.10.2011
Conflicts of interest: None
GIANT TUBERCULOSIS VERRUCOSA CUTIS
Rokon Uddin1, Farzana Akhter2, Abu Baker1
1Department of skin & VD, Enam Medical College & Hospital, Savar, Dhaka, Bangladesh
2Department of skin & VD Upozila Health Complex, Savar, Dhaka, Bangladesh
Corresponding author: Dr. Md. Rokon Uddin e-mail: drrokon47@gmail.com
How to cite an article: Uddin R, Akhter F, Baker A. Giant Tuberculosis Verrucosa Cutis. Our Dermatol Online 2012; 3(1): 21-23.
Abstract
A 38year old man had asymptomatic slowly progressive warty lesion on extensor surface of left elbow and arm for about 20 years. Examination revealed larger one sized of 16cm×15cm and smaller one about 8cm×5cm. Lesions were Keratotic, verrucous, nontender, cauliflower-like indurated plaque. Mantoux test resulted 20mm×18mm on 48 hours observation. Histopathological examination of the lesion showed epitheloid cell granuloma with giant cells and lymphocytes in the mid dermis. The conclusive diagnosis was tuberculosis verrucosa cutis based on above findings. Six month therapy with INH 300mg plus Rifampicin 600mg supplemented initial 2 months ethambulol 1000mg plus pyrazinamide 1500mg daily resulted complete clearance of the lesions.
Key words: skin tuberculosis; tuberculosis verrucosa cutis; gaint
Introduction
Tuberculosis is quite common in Bangladesh. Tuberculosis verrucosa cutis (TVC) occurs from exogenous inoculation of bacilli into the skin of a previously sensitized person with strong immunity against Mycobacterium tuberculosis [1].The tuberculin test is strongly positive. Clinically, the lesion begins as a small papule, which becomes hyperkeratotic, resembling a wart. The lesion enlarges by peripheral expansion, with or without central clearing, sometimes reaching several centimeters or more in diameter [1]. Lesions are almost always solitary, and regional adenopathy is usually present only if secondary bacterial infection occurs. The infection is exogenously acquired and hence the lesions usually appear on exposed or trauma prone areas [2]. A case of accidental infection through throne pricks leading to the lesions which spared gradually for the last 20 years, larger one almost cover the left extensor elbow.
Case Report
A 38 years old man presented with history of asymptomatic, gradually progressing, warty growth, on the back of left elbow and arm for 20 years. The lesions were preceded by thorn pricks. There were no constitutional or systemic symptoms. He did not have any past or family history of tuberculosis. Cutaneous examination revealed keratotic, nontender, cauliflower like indurated plague ranging from 16cm ×15cm to 8cm× 5cm on the back of left elbow and on back of the left arm (Fig. 1,2). There was no lymphadenopathy. Systemic examination was unremarkable. Histopathological examination of the lesion showed pseudoepitheliomatous hyperplasia of the epidermis and a epitheloid cell granuloma having giants cells and lymphocytes in the mid dermis (Fig. 3). Ziehl- Neelson staing of the tissue did not reveal any acid fast bacilli. Mantoux test was positive (20mm×18mm on 2nd day). Hematological investigations revealed a normal haemogram except ESR which was marked as 40mm in 1st hour (Westergren method). Other routine investigations of the blood, urine and stool were unremarkable. Skiagram of the chest showed no abnormality. Based on these clinical features, histopathology and Montoux test, a diagnosis of tuberculosis verrucosa cuits was confirmed. The patient was treated with six month therapy INH 300mg plus Rifampicin 600mg supplemented with initial 2 months ethambulol 1000mg plus pyrazinamide 1500mg daily resulted complete clearence of the lesion. Six months later the histopathological examination of the tissue was done and the result found unremarkable.
 Figure 1. Hyperkeratotic plaque arising at the site of inoculation in an individual
|
 Figure 2. Hyperkeratotic cauliflower like indurated plaque left extensor elbow
|
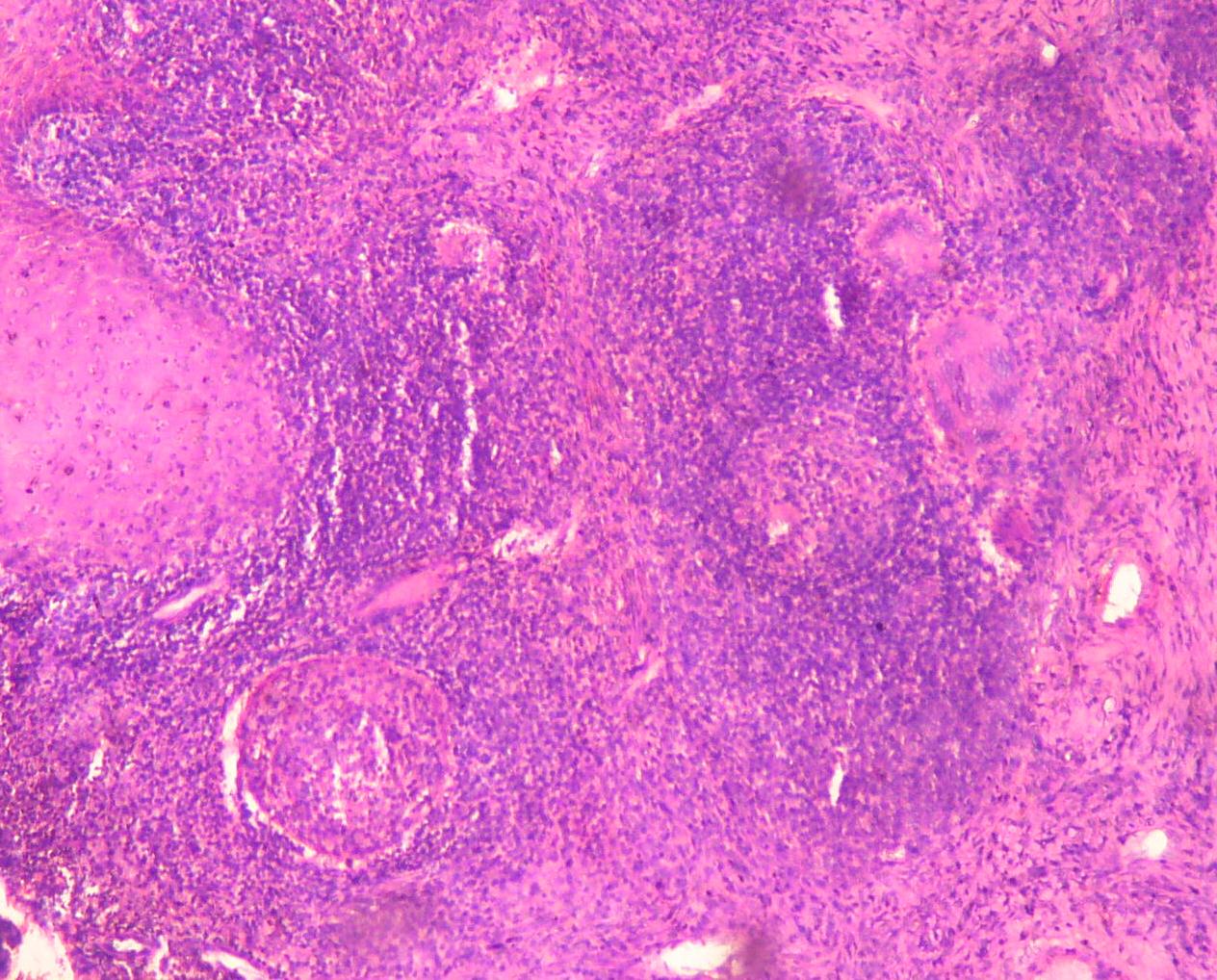 Figure 3. Focus under Zeiss Microscope with Epitheloid cell granuloma having giants cells and lymphocytes in the mid dermis 10 magnificsation
|
Conclusion
TVC patients usually have moderate or high degree of immunity. This patient had positive Mantoux test to support these criteria. The sites which are commonly involved are exposed parts of the body such as fingers, hands, wrists, forearm, arm, ankles, feet, knees, heels and in case of children buttocks [3]. This patient’s lesion was also over the extensor elbow & back of arm- which support the criteria. The man acquired the infection through thorn pricks. Usually TVC begins as small papule and become hyperkeratotic enlarges by peripheral expansion and sometimes reaching several centimeters. This case had cauliflower like lesion about 16cm ×15cm which was quite larger than usual. Complete clearance of warty lesions after the treatment with the anti tubercular regimen composed of INH, Rifampicin, Ethambulol, and Pyrazinamide was strongly suggestive of tubercular etiology.
REFERENCES
1. Janes WD, Berger TG, Elston DM: Andrews’ Disease of the Skin Clinical Dermatology. 10th edition USA: Elsevier 2006; 334-335.
2. Cloides RL: Sir William Osler and the anatomical tubercle. AJ AM Acad Dermatol 1987; 16: 1071-1074.
3. Wolff K, Goldsmith LA, Katz SI, Gilcrest BA, Paller AS, Ieffell DJ: Fitzpatrick’s Dermatology In General Medicine. 7th edition, Vol.2. New York; McGraw Hill, 2008; 1768- 1775.
Comments are closed.