Clinical and histological findings of a typical case of angiolymphoid hyperplasia without eosinophilia: a rare and difficult-to-treat disease
Ivonne Dannesy Rodriguez Hernandez 1, Camila Barreto Vianna Martins1, Luciana Pantaleão2, Maria Claudia Almeida Issa3
1, Camila Barreto Vianna Martins1, Luciana Pantaleão2, Maria Claudia Almeida Issa3
1Post Graduate Student of Dermatology, Universidade Federal Fluminense, Rio de Janeiro, Brazil; 2Department of Pathology, Universidade Federal Fluminense, Rio de Janeiro, Brazil; 3Department of Clinical Medicine, Fluminense Federal University, Rio de Janeiro, Brazil
Corresponding author: Dr. Ivonne Dannesy Rodriguez Hernandez, E-mail: ivonne0788@hotmail.com
Submission: 07.02.2019; Acceptance: 13.04.2019
DOI: 10.7241/ourd.20193.13
Cite this article: Hernandez IDR, Martins CBV, Pantaleão L, Issa MCA. Clinical and histological fi ndings of a typical case of angiolymphoid hyperplasia without eosinophilia: a rare and diffi cult-to-treat disease. Our Dermatol Online. 2019;10(3):275-277.
Citation tools:
BibTex | CSV | RIS | refer/BiblX | Endnote XML | Wikipedia Citation Templates
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Angiolymphoid hyperplasia with eosinophilia (ALHE) is a rare vascular condition characterized by cutaneous papules, plaques or nodules, predominantly located on the head and neck. The main differential diagnosis of ALHE is Kimura’s disease. The treatment is a challenge and the gold standard treatment is surgical excision, as relapse is commonly observed. We report a case of a 57-year-old female with ALHE with an unusual clinical improvement at 2-month follow-up after topical corticosteroid without recurrence 12 months after treatment. Due to its rarity, ALHE can be misdiagnosed. In this case, the characteristic lesions in typical location supported our first clinical diagnose, which was confirmed by histological studies. The clinical improvement after topical steroids without recurrence after long period follow-up caught our attention.
Key words:Angiolymphoid hyperplasia, Vascular, Eosinophilia, Kimura’s disease
INTRODUCTION
Angiolymphoid hyperplasia with eosinophilia (ALHE) is a rare, locally proliferative, benign and idiopathic condition that usually affects middle-aged Caucasian women [1]. ALHE pathogenesis remains unknown, but some authors believe that the lesion originates from a vascular tumor or secondary to vascular damage, such as skin trauma, infections (HTLV or herpes virus 8) or hormonal imbalance [2]. ALHE is characterized by cutaneous papules, plaques or nodules, which may be single or clustered, erythematous, violaceous or brown [3]. It is predominantly located on the head and neck [4]. The absence of eosinophilia is not uncommon, but increased serum Immunoglobulin E (Ig E) can be found.
ALHE and Kimura’s disease were considered for many years the same entity and to this day they are often confused. Both diseases share common clinical and histopathological features. However, it is believed that they are two distinct diseases because of their clinical and histopathology differences [4].
The treatment of choice for ALHE is surgical excision, but relapse is common. Cryotherapy, local radiotherapy, topical or intralesional corticosteroids, imiquimod, acitretin, and laser therapy (dye laser, CO2 laser) are also reported as possible treatments with varying success levels. There are reported cases of spontaneous regression [2].
We report a case of a patient diagnosed with ALHE, without eosinophilia, with good clinical response to topical corticosteroid treatment.
CASE REPORT
A 57-year-old female patient, diagnosed with vitiligo and past history of benign thyroid nodule. She complained about pruritic and painful erythematous-violaceous papules located on the tragus (Fig. 1) for 5 years without treatment. She denied any systemic disease or no chronic use of medicaments. Dermatologic examination: achromatic macules on the anterior thorax, forearms and hands, corresponding to the clinical diagnosis of vitiligo. Red-violaceous nodules grouped on tragus and outer auditive channel. The main diagnostic hypothesis was Angiolymphoid Hyperplasia with Eosinophilia, and differential diagnoses were Kimura’s Disease and Kaposi’s Sarcoma.

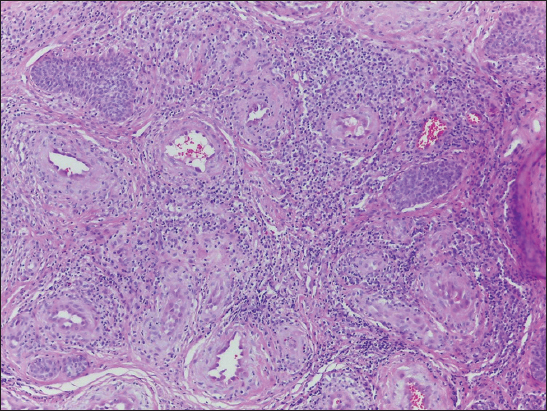
A cutaneous lesion biopsy was performed in the lesion on the left tragus and submitted to histopathological examination, which revealed diffuse inflammatory infiltrate with lymphocytes and eosinophils, hyperplasia of the blood vessels and capillaries with prominent endothelium, confirming the diagnosis of Angiolymphoid Hyperplasia with Eosinophilia (Fig. 2).
Laboratory tests did not show eosinophilia or Ig E alterations. She had anti-TPO antibodies positive in high titers, normal thyroid hormones levels, and normal thyroid ultrasonography. Therefore, topical treatment with mometasone furoate cream, once a day for two months was introduced with the aim of relieving symptoms and avoiding surgery.
DISCUSSION
Clinically ALHE present as persistent or recurrent erythematous or hyperpigmented papules or nodules, usually located in the periauricular area and the scalp [1]. In our case, the patient had erythematous-violaceous papules on tragus and outer auditive channel.
The main differential diagnosis of ALHE is Kimura’s disease. They seem to be the same disease due to the clinical similarity of cutaneous lesions, however most studies now consider them as two different entities. Clinical differences to distinguish Kimura’s disease from ALHE would be a greater diameter of skin lesions, more insidious evolution, and erythematous or purpuric staining of ALHE. This latter characteristic reflects the vascular nature of this process. Kimura’s disease presents clinically with one or more subcutaneous nodules, salivary glands involvement, lymph node enlargement and it is commonly associated with peripheral eosinophilia and IgE elevation [2]. In our case, the patient had only cutaneous lesions consistent with the diagnosis of ALHE.
On histolopathology ALHE disease usually does not resemble lymphoid tissue, it is primarily a disorder of blood vessels and has structures similar to abnormal dilated veins located in the dermis and/or subcutaneous tissue, with abundant mucin deposition on its walls. On the other hand, Kimura’s disease is a disorder of lymphoid follicles, which are predominant feature in large quantities [3]. The histopathological examination of our patient revealed diffuse inflammatory infiltrate with lymphocytes and eosinophils, epithelial hyperplasia of the blood vessels and capillaries with prominent endothelium as described for ALHE disease.
The treatment of ALHE disease is always a challenge. The gold standard is surgical excision, but relapse is common. In our patient, we chose mometasone furoate topically applied once a day. A significant clinical improvement was observed at 2- month follow-up treatment with no relapse 12 months after treatment. (Fig. 3).

CONCLUSION
ALHE is a rare difficult-to-treat condition. The characteristics lesions and locations help diagnosis and complementary exams are necessary to exclude other dermatoses. In our case, the rarity, typical clinical and histological findings and the good clinical response to topical corticosteroid treatment without relapse after a long period follow-up encourage our publication.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Quattrocchi CM, Jankovic R, Jacquier M, Sánchez A, Bergero A, Bussy RAF, [Angiolymphoid hyperplasia with eosinophilia: case report]Arch Argent Dermatol 2012; 62: 189-92.
2. Bastos JT, Rocha CRM, Silva PMC, Freitas BMP, Cassia FF, Avelleira JCR, Angiolymphoid hyperplasia with eosinophilia versus Kimura’s disease: a case report and a clinical and histopathological comparisonAn Bras Dermatol 2017; 92: 392-4.
3. Nogueira A, Acciolly Filho JW, Castro MCR, Maceira JP, Ramos-e-Silva MC, Angiolymphoid hyperplasia with eosinophilia –report of two casesAn Bras Dermatol 2003; 78: 79-85.
4. Briggs PL, Kimura disease is not angiolymphoid hyperplasia with eosinophilia: clinical and pathological correlation with literature review and definition of diagnostic criteriaAn Bras Dermatol 2006; 81: 167-73.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.