Piccardi-Lassueur-Graham-Little syndrome associated with frontal fibrosing alopecia and lichen planus pigmentosus
Selma El Kadiri , Hanane Baybay, Rhizlane Chaoui, Zakia Douhi, Sara Elloudi, Fatima Zahra Mernissi
, Hanane Baybay, Rhizlane Chaoui, Zakia Douhi, Sara Elloudi, Fatima Zahra Mernissi
Department of Dermatology, University Hospital Hassan II, Fez, Morocco
Corresponding author: Dr. Selma El Kadiri
Submission: 13.04.2020; Acceptance: 30.06.2020
DOI: 10.7241/ourd.2020e.64
Cite this article: El Kadiri S, Baybay H, Chaoui R, Douhi Z, Elloudi S, Mernissi FZ. Piccardi-Lassueur-Graham-Little syndrome associated with frontal fi brosing alopecia and lichen planus pigmentosus. Our Dermatol Online. 2020;11(e):e64.1-e64.2.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
A 51-year-old postmenopausal woman presented with history of progressive hair loss over the scalp, axilla, groin and eye-brows since 3 years. Over the same period, she had noticed a darkening and mild itch on the face. However her past medical history was unremarkable.
Dermatological examination revealed a plaque of cicatricial alopecia on the scalp with a 2-cm band of recession along the frontotemporal hairline; the underlying skin was smooth and shiny (Fig. 1). Loss of eye-brows was noted (Fig. 2). Non-scarring alopecia was present over the axillar and pubic regions (Figs. 3a and 3b). Multiple follicular papules over the thighs were observed (Fig. 4). Finally gray-brown pigmented patches,non atrophic,smooth in surface with a reticular pattern located on the forehead, nose,periorbital region and cheeks were present (Fig. 5).
 |
Figure: 1 Plaque of cicatricial alopecia on the scalp with a recession of the frontotemporal hairline. |
|
Figure: 2 Loss of eye-brows |
 |
Figure: 3 (a and b) Non-scarring alopecia was over the axillar and pubic regions. |
 |
Figure: 4 Multiple follicular papules over the thighs. |
 |
Figure: 5 Confluent gray-brown pigmented patches, involving forehead, nose, periorbital region and cheeks. |
On dermoscopy, an exaggerated pseudoreticular pigmentary network with grey Perifollicular globules was noted for the lesion of face, while dermoscopy of the scalp showed follicular hyperkeratosis (Figs. 6a and 6b).
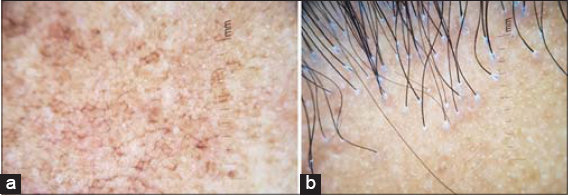 |
Figure: 6 a) Dermoscopy of the face demonstrated an exaggerated pseudoreticular pigmentary network with gray perifollicular globules; b) Dermoscopy of the scalp with perifollicular hyperkeratosis. |
However nails, mucosa, palms and soles were normal.
Piccardi-Lassueur-Graham-Little syndrome associated with frontal fibrosing alopecia and lichen planus pigmentosus was diagnosed.
Blood tests including thyroid hormone profile, autoimmune tests, and viral serologies, were normal.
The patient was prescribed oral corticosteroid at a dose of 60 mg once daily (1 mg/kg), and measures of sunscreen for 3 months with partial improvement.
The Piccardi-Lassueur-Graham-Little syndrome (PLGLS) first reported by Piccardi, in 1913, is a rare disorder, characterized by the triad of multifocal scarring alopecia of the scalp, keratotic follicular eruption and noncicatricial alopecia of the axilla and groin [1]. It’s etiology remains unclear, but studies focusing on clinical, histological, and immunofluorescent features of PLGLS suggest that it could be a variant of lichen planopilaris [2]. Patients may present at least one episode of lichen planus or mucosa during the course of the disease [1].
Frontal fibrosing alopecia (FFA) is a primary lymphocytic scarring alopecia with a distinctive clinical pattern of progressive frontotemporal hairline recession and eyebrow loss that preferentially affects the postmenopausal women [3]. It’s association with PLGLS still rarely described and uncommon.
Lichen planus pigmentosus (LPPig) is a rare variant of classic lichen planus of unclear etiology that tends to occur in middle-aged individuals with skin types III to VI [4].
To our knowledge, we report a rare association between Piccardi-Lassueur-Graham-Little syndrome, frontal fibrosing alopecia and lichen planus pigmentosus which its common pathogenic mechanism remains unclear.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
REFERENCES
1. Steglich RB, Tonoli RE, Pinto GM, Müller FM, Guarenti IM, Duvelius ES. Graham-Little Piccardi Lassueur syndrome:case report. An Bras Dermatol. 2012;87:775-7.
2. Rawat R, Mahajan VK, Chander B, Mehta KS, Chauhan PS, Gupta M. Graham Little Picardi Lassueur syndrome. Our Dermatol Online. 2016;7:114-6.
3. Piotrkowicz M, Owczarek W. Frontal fibrosing alopecia and ulerythema ophryogenes as two entites that can transist one into another. Our Dermatol Online. 2018;9:290-93.
4. Takeoka S, Tada Y, Ohnishi T, Watanabe S. Case of lichen planus pigmentosus with unique distribution. J Dermatol. 2015;42:652–4.
Notes
Source of Support: Nil.
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/000-0003-3455-3810 http://orcid.org/000-0003-3455-3810 |

Comments are closed.