When dermoscopy facilitate diagnosis of lichen planus pigmentosus
Rhizlane Chaoui , Selma El Kadiri, Asmae Rasso, Zakia Douhi, Sara Elloudi, Hanane Baybay, Fatima Zahra Mernissi
, Selma El Kadiri, Asmae Rasso, Zakia Douhi, Sara Elloudi, Hanane Baybay, Fatima Zahra Mernissi
Department of Dermatology, University Hospital Hassan II, Fez, Morocco
Corresponding author: Dr. Rhizlane Chaoui
Submission: 15.03.2020; Acceptance: 09.04.2020
DOI: 10.7241/ourd.2020e.48
Cite this article: Chaoui R, El Kadiri S, Rasso A, Douhi Z, Elloudi S, Baybay H, Mernissi FZ. When dermoscopy facilitate diagnosis of lichen planus pigmentosus. Our Dermatol Online. 2020;11(e):e48.1-e48.2.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
A 51-year-old female presented with asymptomatic brownish patches on the face and neck of two year’s duration. She was otherwise healthy, no history of exposure to drugs or using cosmetics prior to onset of the lesions could be elicited.
Dermatological examination revealed gray-brown pigmented macules,scaly, non atrophic, smooth in surface, confluent, forming pigmented patches with a reticular pattern extensively involving forehead, nose, chin, perioral region, neck and sparing the cheeks (Figs. 1a – 1d).
 |
Figure 1: (a-d) Confluent gray-brown pigmented macules and patches, involving forehead, nose, chin, perioral region, neck and sparing the cheeks. |
However, her nails, hair, mucosa, palms and soles were normal.
In front of this clinical presentation we thought about many diagnosis such us lichen planus pigmentosus, macular amyloidosis and ashy dermatosis.
On dermoscopy, we demonstrated exaggerated pseudoreticular pigmentary network with grey Peririfollicular globules and dots (Figa. 2a and 2b).
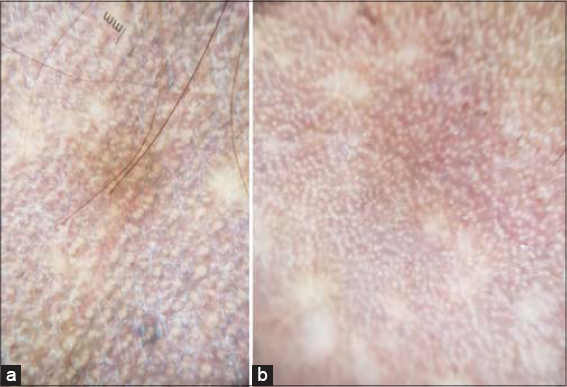 |
Figure 2: (a and b) Dermoscopy demonstrated an exaggerated pseudoreticular pigmentary network with gray perifollicular globules and dots. |
Finally, the diagnosis of lichen planus pigmentosus was made.
Routine laboratory data including blood cell count and serology for hepatitis B and C were normal.
The patient was prescribed topical steroid once daily, and measures of sunscreen for 4 months with partial improvement.
Lichen planus pigmentosus (LPPig), is a chronic inflammatory pigmentary disorder that first described by Bhautani et al. [1]. It is an uncommon variant of classic lichen planus of unknown etiology that tends to occur in middle-aged individuals with skin types III to VI [2].
Clinically, it has been characterized by hyperpigmented, dark brown macules in a diffuse, blotchy, reticular, or perifollicular pattern involving the sun-exposed areas and flexural folds including the axillary, inguinal, and submammary regions [3].
The mucous membrane, scalp, palms, soles, nail are rarely involved [4].
Dermoscopy is a non invasive tool that can help with diagnosis of lichen planus pigmentosus and will show different features including exaggerated pseudoreticular network, gray-brown or gray-blue perifollicular globules and dots, blotches, rods and white lines. Vascular changes might be found in some cases [5].
There are no established treatments for LPP, but generally treatment consists of topical steroids, tacrolimus, depigmenting agents (Topical agents include hydroquinone often in combination with retinoic acid, azelaic acid, kojic acid and glycolic acid), photoprotection, and Q-switched Nd-YAG laser [6].
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
REFERENCES
1. Bhutani LK, Bedi TR, Pandhi RK, Nayak NC. Lichen planus pigmentosus. Dermatologica. 1974;149:43–50.
2. Takeoka S, Tada Y, Ohnishi T, Watanabe S. Case of lichen planus pigmentosus with unique distribution. J Dermatol. 2015;42:652–4.
3. Rieder E, Kaplan J, Kamino H, Sanchez M, Pomeranz MK. Lichen planus pigmentosus. Dermatol Online J. 2013;19:20713.
4. Lambertini M, Patrizi A, Ravaioli GM, Dika E. Oral pigmentation in physiologic conditions, post-inflammatory affections and systemic diseases. G Ital Dermatol Venereol. 2018;153:666-71.
5. Sonthalia S, Errichetti E, Kaliyadan F, Jha AK, Lallas A. Dermoscopy of lichen planus pigmentosus in Indian patients –Pitfalls to avoid. Indian J Dermatol Venereol Leprol. 2018;84:311-3.
6. Al-Mutairi N, El-Khalawany M. Clinicopathological characteristics of lichen planus pigmentosus and its response to tacrolimus ointment:an open label, non-randomized, prospective study. J Eur Acad Dermatol Venereol. 2010;24:535–40.
Notes
Source of Support: Nil.
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

 http://orcid.org/000-0003-3455-3810
http://orcid.org/000-0003-3455-3810
Comments are closed.