Systemic anaplastic large cell lymphomas ALK negative revealed by a skin mass
Rhizlane Chaoui , Sara Elloudi, Selma El Kadiri, Zakia Douhi, Hanane Baybay, Fatima Zahra Mernissi
, Sara Elloudi, Selma El Kadiri, Zakia Douhi, Hanane Baybay, Fatima Zahra Mernissi
Department of Dermatology, University Hospital Hassan II, Fez, Morocco
Corresponding author: Dr. Rhizlane Chaoui
Submission: 08.03.2020; Acceptance: 12.06.2020
DOI: 10.7241/ourd.2020e.40
Cite this article: Chaoui R, Elloudi S, El Kadiri S, Douhi Z, Baybay H, Mernissi FZ. Systemicanaplastic large celllymphomas ALK negativerevealed by a skin mass. Our Dermatol Online. 2020;11(e):e40.1-e40.3.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Anaplastic large cell lymphomas (ALCLs) are T-cell lymphomas that express CD30. Clinically, ALCL has 2 presentations: the systemic formand the primary cutaneous form. We report a case of ALK negative systemic anaplastic large cell lymphomas revealed by a skin tumor. Complete staging is mandatory in ALCL especially in cases of abnormal skin manifestation with ALK negative to discriminate a primary cutaneous ALCL from sALCL secondarily involving the skin
Key words: Anaplastic large cell lymphoma; ALK-negative; Extranodal
INTRODUCTION
Anaplastic large cell lymphomas (ALCLs) are T-cell lymphomas that express CD30 [1]. Clinically, ALCL has 2 presentations: the systemic formand the primary cutaneous form [2].
We report a case of ALK negative systemic anaplastic large cell lymphomas revealed by a skin tumor.
CASE REPORT
A 76-year-old male,complained of an asymptomatic erythematous lesion on the fold of the right elbow that has been ongoing for a 6 months ago.The lesion is gradually increasing in size.Five months laterthe patient reported similar lesions at the periphery of the initial lesion.The patient was in otherwise good health without any significant past medical history.
Dermatological examination revealed awell demarcated tumor, erythematous in color,5 cms in diameter,hard in consistency with a smooth surface involving the fold of the right elbow (Figs. 1a and 1b). The lesion was adhered to the deep plans.Multiple erythematous papules,varying in size were noted at the periphery of the lesion described above (Fig. 2).
 |
Figure 1: (a and b) Well defined tumor, erythematous in color, 5 cms in diameter,with a smooth surface located on the fold of the right elbow. |
 |
Figure 2: Multiple erythematous papules, varying in size at the periphery of the tumor. |
On dermoscopy, we observed telangiectasias with arborizing vessels (Fig. 3).
 |
Figure 3: Dermoscopy showingtelangiectasias with arborizing vessels. |
Axillary examination showed multiple lenticular right axillary lymph nodes.However the abdomen was soft and no hepatosplenomegaly was noted.
In front of this clinical presentation we thought about many diagnosis such us mycosis fungoides, B lymphoma,sarcoma and skin metastasis.
A skin biopsy was performed and histopathological examination revealeda dense dermal lymphoid infiltrate consisting of large atypical CD30+ T cells (CD45+ CD4+ CD5+ CD30+ CD3- CD8-ALK1–) with an anaplastic morphology and high proliferation rate.
These findings, in correlation with clinical features were suggestive of anaplastic large cell lymphoma (ALCL).
Complete staging was performed to assess systemic disease. Laboratory tests were unremarkable.Lymph node ultrasound revealed a malignant lymphadenopathy at the right axillary measuring 5.4 mm of small axis.A biopsy was performed showing a lymph node location of anaplastic large cell lymphoma.Computed tomographyscan of the neck, chest, abdomen, and pelvis was normal.
The patient was treated with CHOEP (cyclophosphamide, doxorubicin, vincristine, etoposide and prednisone) regimen to a total of six sessions, which resulted incomplete clearance of cutaneous(Figs. 4a and 4b) and axillary lymph nodes lesions.No recurrence was noted 12 months later.
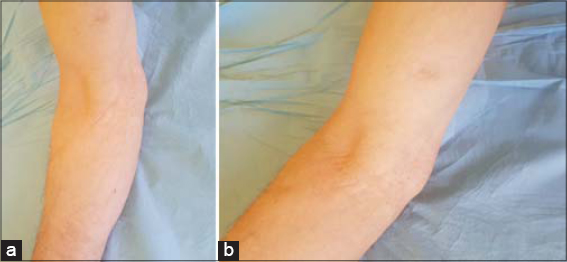 |
Figure 4: (a and b) Complete clearance of the cutaneous lesions. |
DISCUSSION
Anaplastic large cell lymphomas (ALCLs) comprise a heterogeneous group of relatively rare T-cell non-Hodgkin lymphomas that are characterized by CD30 expression [1]. Clinically, ALCL has 2 distinct presentations. The systemic form usually involves lymph nodes with/without extranodal sites and which has a poor prognosis,the primary cutaneous form is restricted to the skin and is characterized by an excellent prognosis with a 5-year overall survival (OS) of 90% [2].
Systemic ALCL (sALCL) is further divided into ALK-positive and ALK-negative subtypes, depending on the expression of the anaplastic lymphoma kinase (ALK) fusion protein [3]. ALK positive ALCLs occur predominantly in children and young adults, ALK-negative ALCLs, affect older adults with a median age at diagnosis of approximately 55–60 years.Male predominance (60%) is seen in both ALK+ and ALK- subtypes [4].
However, ALK protein expression, can be helpful for differentiating between systemic (ALK positive in 80% of cases) and primary cutaneous anaplastic large cell lymphoma(ALK negative in 100% of cases) and aid in therapeutic decision [4].
sALCL is primarily a nodal disease, though extranodal involvement is seen in ~20% of cases. The skin,liver, lungs, bone and bone marrow areespeciallyextranodal sites of involvement [4,5]. Skin involvement is not rare, and often manifests as masses, multiple nodules or nonhealing ulcers [6]. It was important to stage patients with skin lesions to differentiate primary cutaneous ALCL from sALCL secondarily involving the skin [7].
ALCLs are diagnostically challenging for the pathologists,histologically, cellswere large and pleomorphicwith eccentric horseshoe-shaped nuclei knows as “hallmark” cells. These cells typically form sheets of neoplastic cells effacing the nodal architecture, mimicking metastatic involvement from carcinoma [8].
Immunohistochemistry (IHC) is essential in the diagnosis and subclassification of ALCL. In ALCLs all tumour cells are strongly and equaly positive for CD30, usually at the cell membrane and in the Golgi region.However, it must keeping in mind that CD30 expression is not specific for ALCL and can be expressed in classical hodgkin lymphoma, peripheral T-cell lymphoma-not otherwise specified (PTCL-NOS) being the main differential diagnoses [8].
The neoplastic cells in both ALK+ and ALK- sALCL often lack expression of one or more pan-T-cell antigens, including CD3, CD5, CD7, and CD8. CD2 and CD4 are the T-cell antigens most often expressed [9].
Complete staging and work-up for ALCL includes an accurate physical examination, complete haematological and biochemical exams, total-body computerized tomography, and bone marrow aspirate and biopsy [10].
The treatment of choice for systemic ALCL, whether ALK-positive or ALK-negative, is polychemotherapy. Because of the poor prognosis.
Auto-peripheral blood stem cell transplantation is suggested for treatment in patients with complete response to chemotherapy [11].
CONCLUSION
Complete staging is mandatory in ALCL especially in cases of abnormal skin manifestation with ALK negative to discriminate a primary cutaneous ALCL from sALCL secondarily involving the skinand to make the correct choice of treatment and evaluation of prognosis.
Consent
The examination of the patient wasconductedaccording to the Declaration of Helsinki principles.
The authorscertifythatthey have obtained all appropriate patient consent forms. In the form the patient(s) has/have givenhis/her/their consent for his/her/their images and otherclinical information to bereported in the journal. The patients understandthattheirnames and initialswill not bepublished and due efforts willbe made to concealtheiridentity, but anonymitycannotbeguaranteed.
REFERENCES
1. Parrilla Castellar ER, Jaffe ES, Said JW, Swerdlow SH, Ketterling RP, Knudson RA, et al. ALK-negative anaplastic large cell lymphoma is a genetically heterogeneous disease with widely disparate clinical outcomes. Blood. 2014;124:1473-80.
2. Medeiros LJ, Elenitoba-Johnson KS. Anaplasticlarge celllymphoma. Am J Clin Pathol. 2007;127:707–22.
3. Abdull Gaffar B, Seliem RM. ALK-Negative Anaplastic large cell lymphoma presenting as an extranodal soft-tissue mass with an unusual alveolar growth attern:A diagnostic challenge. Int J Surg Pathol. 2017;25:502–6.
4. Falini B, Pileri S, Zinzani PL, Carbone A, Zagonel V, Wolf-Peeters C, et al. ALK+lymphoma:clinico-pathological findings and outcome. Blood. 1999;93:2697-706.
5. Gascoyne RD, Aoun P, Wu D, Chhanabhai M, Skinnider BF, Greiner TC, et al. Prognostic significance of anaplastic lymphoma kinase (ALK) protein expression in adults with anaplastic large cell lymphoma. Blood. 1999;93:3913-21.
6. Bennani-Baiti N, Ansell S, Feldman AL. Adult systemic anaplastic large-cell lymphoma:recommendations for diagnosis and management. Expert Rev Hematol. 2016;9:137-50.
7. Kempf W, Pfaltz K, Vermeer MH, Cozzio A, Ortiz-Romero PL, Bagot M, et al. EORTC, ISCL, and USCLC consensus recommendations for the treatment of primary cutaneous CD30-positive lymphoproliferative disorders:lymphomatoid papulosis and primary cutaneous anaplastic large-cell lymphoma. Blood. 2011;118:4024-35.
8. Ferreri AJ, Govi S, Pileri SA, Savage KJ. Anaplastic large cell lymphoma, ALK-negative. Crit Rev Oncol Hematol. 2013;85:206-15.
9. Jaffe ES, Nicolae A, Pittaluga S. Peripheral T-cell and NK-cell lymphomas in the WHO classification:pearls and pitfalls. Mod Pathol. 2013;26 Suppl 1:S71-87.
10. Yu X, Zhang J, Xu K, Li M, Yao Z. Skin involvement as the first symptom of rapidly progressive ALK-positive systemic anaplastic large cell lymphoma. Clin Exp Dermatol. 2017;42:539-42.
11. Vu K, Ai W. Update on the Treatment of anaplastic large cell lymphoma. Curr Hematol Malig Rep. 2018;13:135-41.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/000-0003-3455-3810 http://orcid.org/000-0003-3455-3810 |

Comments are closed.