Cystic acne in women who present excess of testosterone because of social reasons and not of pathological diseases. An attempt to treat this malaise by natural remedies and the discovery of a suggestive equation to solve to know how many days of treatment are required for remission
Piotr Brzeziński1, Lorenzo Martini2
¹Institute of Biology and Environmental Protection, Pomeranian Academy, Slupsk, Poland, ²Department of Pharmaceutical Biotechnologies, University of Siena, Italy
Corresponding author: Lorenzo Martini, M.Sc., E-mail: martinil163@libero.it
Submission: 11.01.2018; Acceptance: 25.03.2018
How to cite this article: Brzezinski P, Martini L. Cystic acne in women who present excess of testosterone because of social reasons and not of pathological diseases.An attempt to treat this malaise by natural remedies and the discovery of a suggestive equation to solve to know how many days of treatment are required for remission. Our Dermatol Online. Our Dermatol Online. 2018;9(e):e2.
ABSTRACT
Aims of our research is to demonstrate that by the same way women who have high testosterone levels show always an elevate sex drive, women who indeed have a high sex drive (often because they cannot have regular sexual intercourses with men or are forced to live and work in competitive fields, as Army or prisons or monasteries) have always high testosterone levels.
Excess of testosterone in woman (more than 0.8ng/ml) may lead to cystic acne and our purpose is to treat cystic acne in this type of women, endowed by elevated serum testosterone levels.
Key words: Testosterone; Cystic acid; DHT; Pygeum africanum; Calcium chloride
INTRODUCTION
Some AA refer that there are cases where women have increased testosterone levels, and this can cause a high sex drive in those women, and scope of this study is to demonstrate that,vice versa, high sex drive in female may lead to an appreciable raise of blood testosterone levels and try to explain what may happen in female when testosterone levels are high, especially as far as cystic and ribelle acne is concerned.
Women presenting highest testosterone levels are more competitive, more risk-taking, and more socially dominant, if they are affected by high levels of sex hormones (testosterone but even estradiol). Surprisingly, the hormone that plays the clearest role in female social competition, and in feminine lust, is not an estrogen, but an androgen – testosterone [1].
These phenomena turn out to have many practical applications. For instance, women have higher testosterone levels in societies or clans or équipes where they compete with each other in the work place. This means that they are more sexually liberated and behave more like men in relation to drug use, reckless conduct, and crime. Indeed, their body shape becomes more masculine.
This is the reason why we have recruited 9 volunteers, nine security guards who are female and have to combat everyday and impose themselves upon an avalanche of males.
We want to recall too that abnormally high testosterone levels in women can lead to a variety of symptoms. Most often, women with high testosterone levels develop male pattern hair growth (hirsutism), especially on their faces and chests. More rarely and over time, some women may experience virilization, which is increased muscle mass, redistribution of body fat, enlargement of the clitoris, deepening of the voice, male pattern baldness, cystic acne, and/or increased perspiration [2]. It is welknown that oestrogen, progesterone, and testosterone are hormones that affect a woman’s sexual desire and functioning.
When it comes to sexual desire [3] the most influential hormone is testosterone. Though it’s often considered a male hormone, testosterone — like estrogen– is present in both men and women, though the proportions differ between the sexes (normal women present 10 times less than in men and thus their normal values are comprised between 0.06ng/ml and 0.82ng/ml) [2].
Too much often females present high pools of testosterone because of pathological disease, like:
Insulin Resistance; Estrogen/Progesterone Imbalances (PMS/PMDD, with Estrogen dominance); Lack of Exercise (especially weight training); Adrenal Disease (High DHEA Levels); High Leptin Levels (AKA Leptin Resistance)(keeping on account that Leptin is the hormone that just may be making it impossible for the woman to lose weight and keep it of); Weight gain or Obesity; Oligomenohrrea.
First of all, it must be stressed even that having low progesterone in relation to oestrogen can lead to acne by way of increasing insulin which can lead to excess of androgens, as well as amplify testosterone and thus DHT conversion in the skin.
DHT is a potent acne causing form of testosterone that other forms of testosterone get converted into in the skin via an enzyme called 5-alpha reductase. On the other hand, having a normal progesterone level in relation to estrogen can prevent 5-alpha-reductase from converting testosterone to DHT, which will, in turn, prevent acne.
Increasing progesterone in females who present low level of progesterone and high levels of testosterone is forbidden, dermal cosmeticologically speaking, since topical usage of hormons has been banned from 1986 all over the world.
The suggestion of administering phytoprogesterones could be an optimal solution, even if these types of natural hormones can be retrieved only in food and dermatologists cannot indicate to assume certain food (even if they may suggest food supplements).
For instance, walnut leaf, or Juglans regia, extract and dried leaves are excellent to make teas in order to increase levels of progesterone, all food containing Zinc, as red meat, shellfish, turkey:all these aliments can contribute to increasing the levels of progesterone in the body.
Yam or wild yam contains certain phytochemicals which act like progesterone when inside the body. However, these yams are not to be confused with sweet potatoes, which are also called yams in some areas.
Many Vitamin B6 Rich Foods such as walnuts, whole grains, fortified cereals, and soy milk.
It must be considered that women with too high levels of progesterone, has very low sex drive though, and common causes are when they are in the second phase of the menstrual cycle, or are oligomenorrheic, or are in pre-menopausal phase or have not had their first menarche.
Another option could be to administer orally plants that are recognized to act as exceptional 5 alpha reductase, but only physicians can do it: plants like: Spearmint tea (Mentha spicata); Red reishi, (Genoderma lucidum); Licorice (Glycerrhyza glabra); Chinese peony (Paeonia lactiflora); Black cohosh (Actaea racemosa); Chaste tree (Vitex agnocastus).
And finally a dermatologist can suggest the topical usage of these plants that have a recognized activity as 5 alpha reductase when applied topically.
Polygonum multiflorum for the fact that contains resveratrol-like Stilbenoids.
Black Pepper leaf extract (Piper nigrum); Red Stinkwood (Pygeum africanum); Saw Palmetto ;Serenoa repens, where the active substance possibly is the lauric acid
Pine (Pinus sp. resin,ehere the active substance can be abietic acid); Bitter root (Sophora flavescens); Japanese hedge parsley (Torilis japonica); Northern Whitecedar (Thuja occidentalis).
MATERIAL AND METHODS
We have decided to apply the lotions (that constitute the real treatment) only in the second part of the menstrual cycle of the 9 volunteers, since this is the progestinic phase, when acne is more fierce and boisterous.
All the nine volunteers do not suffer from Insulin Resistance, Estrogen/Progesterone Imbalances, Lack of exercise, Adrenal Disease, obesity or polycystic ovary.
As the typical length of time between the first day of one menstrual period and the first day of the next is 21 to 45 days in young women and the 14th (in rare case the 12nd or the 16th) day is to be considered in all mammals (female) the day that indicates the ovulation and the beginning of bleeding (phenomenon that lasts 3-4 days) and that after this period there is the second phase, the progestinic, we can calculate the days of treatment necessary to remission of the acne, acting like this: if we consider the 14th day the apex of the entire phenomenon of menstruation, we add 4 days more of bleeding and the average of days of the second phase of the cycle is comprised between 4 and 27 days and so the whole duration of the treatment has been chosen of about 15 days.
The treatment must last almost 15 days, corresponding to the progestinic phase of the menstruation [6].
A pre-tratment with a catheretic agent at low percentage (acqueous solution of Calcium chloride 1.5%) to spread on the face skin all the morning.
Generally, eschars appear at the 3rd day, but the action “désinfiltrante” of Calcium ion, let them be dry and fluffy and treatment with the second lotion results less urticant and insidious.
The pre-treatment must be continued till eschars disappear and only pinkish spots remain on skin.
This depends on the type, phototype and colour of individual’s skin.
The very treatment is based on a magma (idest a hydro-glyceric-alcoholic suspension of plant extracts, apt to inhibit 5alpha reductase and we have chosen and prepared in a mix made as follows:
Pine (Pinus sibiricus glyceric extract), Pygeum africanum (dried extract in alcohol) and Black Pepper (Piper cubeba) leaves glyceric extract.
The magma must be applied after seven hours from the pre-treatment.
First of all, we had to evaluate the pool of testosterone in the 9 volunteer owing to a questionnaire based on two simplest questions:
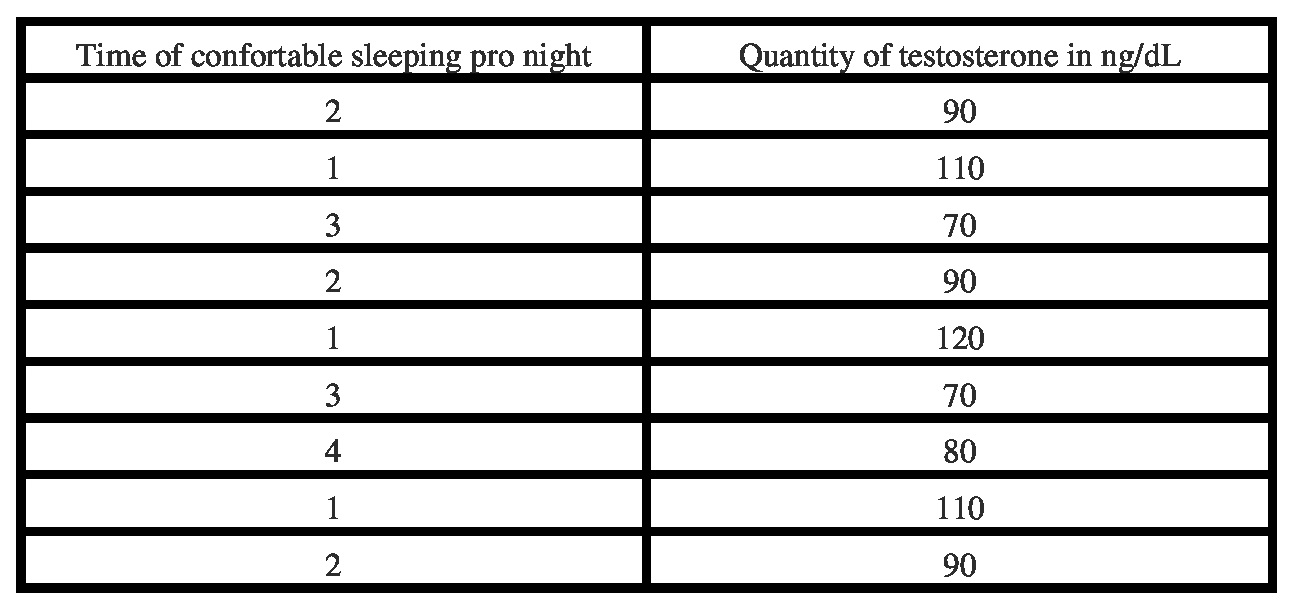
1) How many hours can the volunteer sleeps pro night (considering regular a cycle of 7 hours of uninterrupted sleeping)
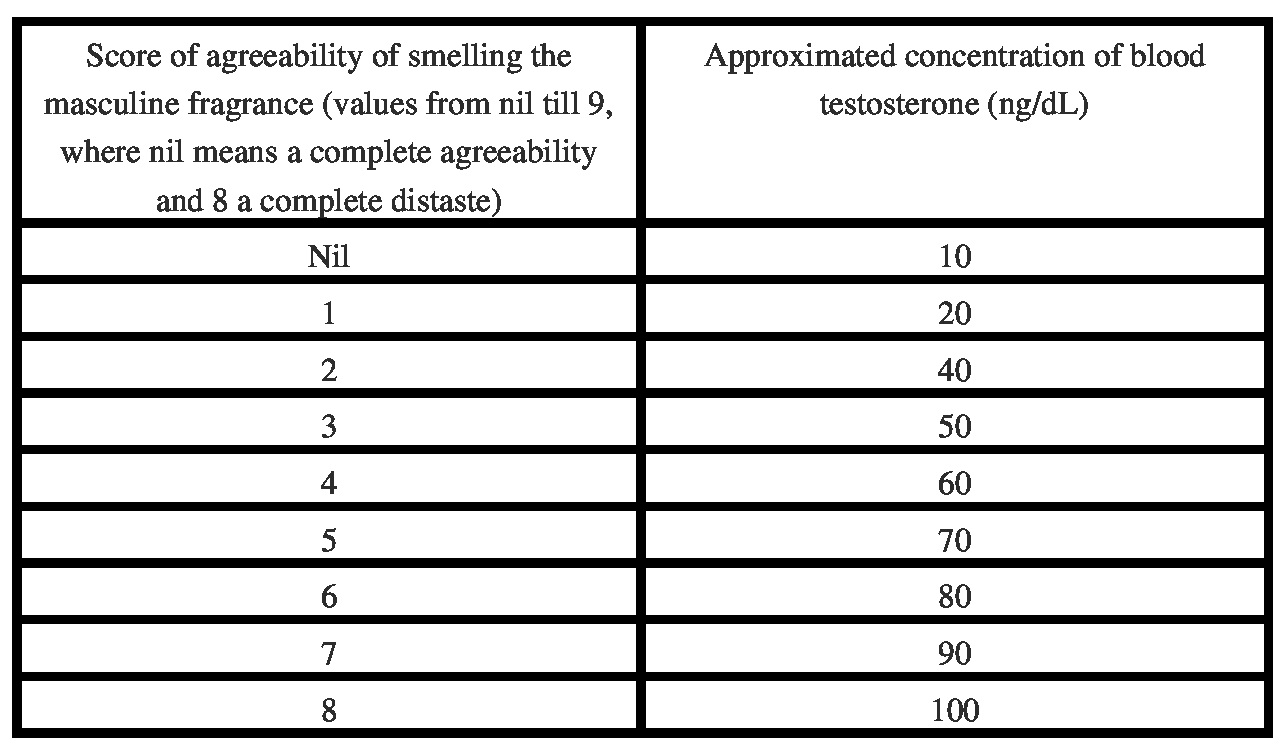
2) Asking to the volunteer, after having let smell a mix of fragrances made up of male secretions (civet, castoreum and musk) if she dislikes or likes the fragrance:this is due to pheromonal phenomena. Male dislikes odour of other male and prefers the odour of female, evoked by estrogens especially during ovulation, and female feels distaste for female’s odour, by the same reason.
The questionnaire is based on studies effectauted by Weary Dunlop – military surgeon in World War II, leader attendant at the Victorian College of Pharmacy, now Monash Parkville Campus, Australia).
In tables 1 and 2, the former where the pool of blood testosterone in woman is evaluated thanks to the hours of well-sleeping pro/night, the latter where the concentration of testosterone in blood is calculated approximatively according to the feeling of distasting of the scent of masculine fragrance, that contains androstenol.
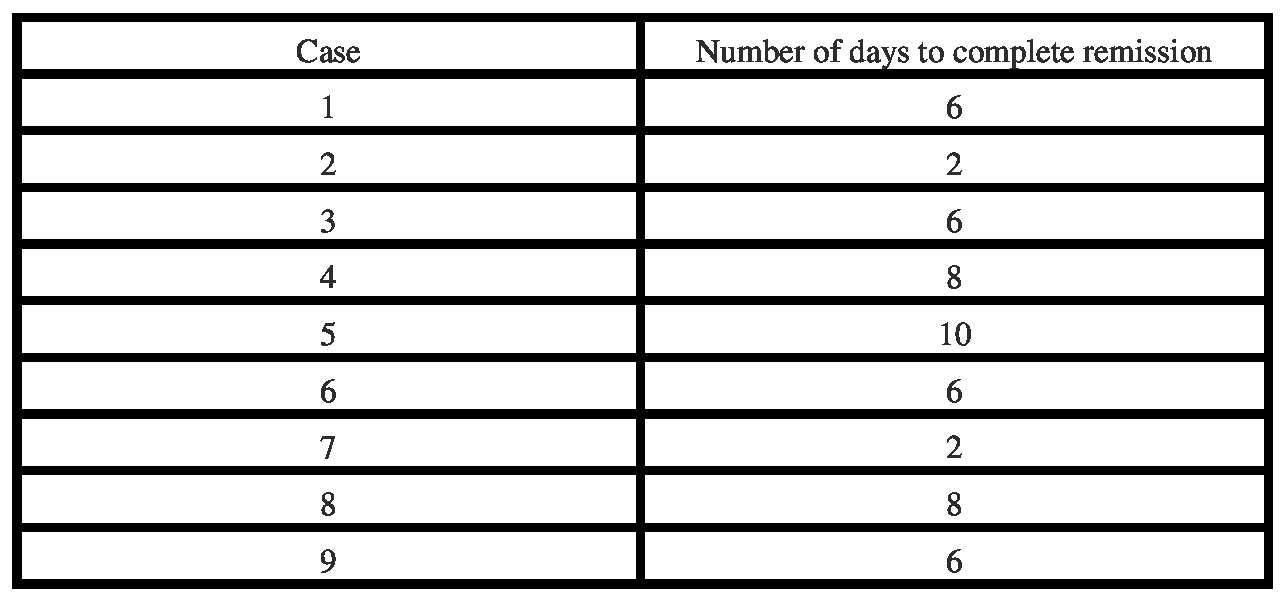
Days required to complete remission = (score of agreeability x 2) + 2
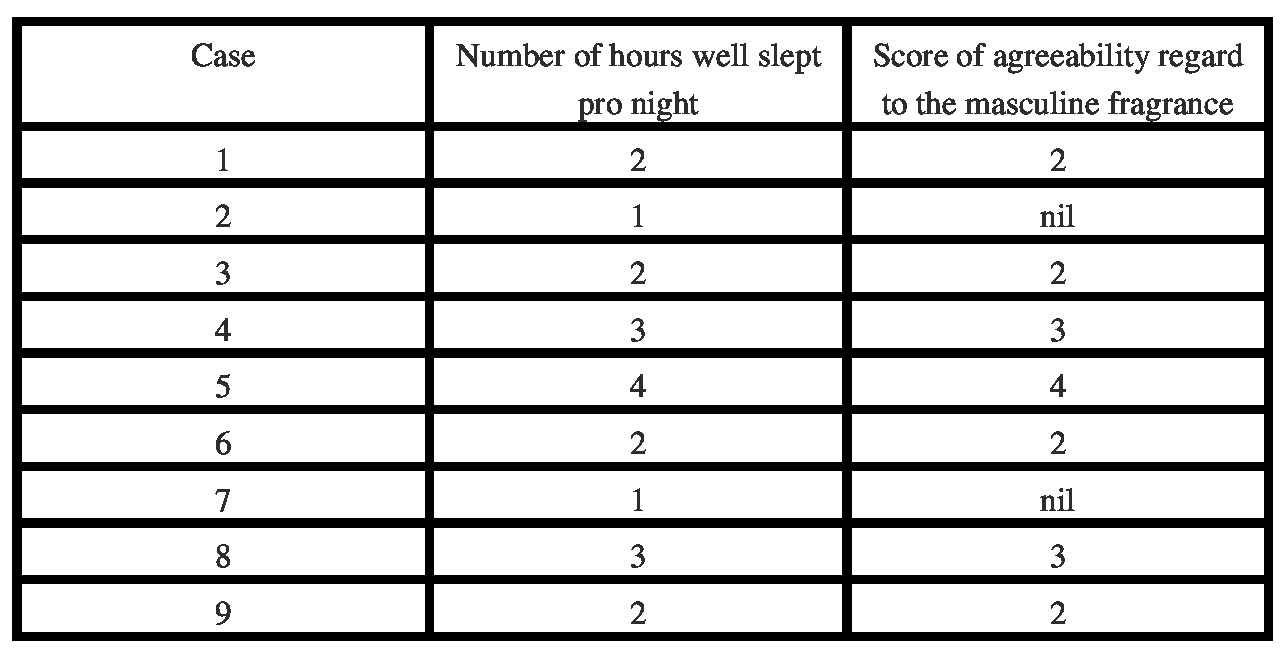
Even very suggestive is Table III, as we had already told, where it can be observed that the same women who sleep a certain number of hours pro night, show the same appreciation for the masculine fragrance.
REFERENCES
1.Barber N. Sex Hormones and Womanly Passions: Competition among women linked to testosterone: Psichology Today. July 28, 2009.
2. Hahn AC, DeBruine LM, Fisher CI, et al. The reward value of infant facial cuteness tracks within-subject changes in women's salivary testosterone. Horm Behav. 2015; 67: 54-59.
3. Wallwiener S, Müller M, Doster A, et al. Sexual activity and sexual dysfunction of women in the perinatal period: a longitudinal study. Arch Gynecol Obstet. 2017; 295: 873-883.
4. Lara LADS, Scalco SCP, Troncon JK, et al. A Model for the Management of Female Sexual Dysfunctions. Rev Bras Ginecol Obstet. 2017; 39: 184-194.
5.Marshall C, Guendelman S, Mauldon J, et al. Young Women's Contraceptive Decision Making: Do Preferences for Contraceptive Attributes Align with Method Choice? Perspect Sex Reprod Health. 2016; 48: 119-127.
6.Judd HL, Yen SS. Serum androstenedione and testosterone levels during the menstrual cycle. J Clin Endocrinol Meta. 1973; 36: 475-481.
7.Andersen ML, Alvarenga TF, Mazaro-Costa R, et al. The association of testosterone, sleep, and sexual function in men and women; Brain Res. 2011 Oct 6;1416:80-104.
8.Fears TR, Ziegler RG, Donaldson JL, et al. Reproducibility studies and interlaboratory concordance for androgen assays in female plasma. Cancer Epidemiol Biomarkers Prev. 2000; 9: 403-412.
9. van Anders SM, Goldey KL. Testosterone and partnering are linked via relationship status for women and 'relationship orientation' for men. Horm Behav. 2010; 58: 820-826.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.