Painful nevus on the left cheek-a case report and discussions
Alin Laurentiu Tatu
Faculty of Medicine and Pharmacy, University ,,Dunarea de Jos “, Galati, Romania
Corresponding author: Alin Laurentiu Tatu, MD PhD, E-mail: dralin_tatu@yahoo.com
Submission: 03.03.2017; Acceptance: 10.03.2017
DOI: 10.7241/ourd.2017e.6
How to cite this article: Tatu AL. Painful nevus on the left cheek-a case report and discussions. Our Dermatol Online. 2017;8(1e):e7.
This dome shaped light brown lesion from the left cheek area of a 29 years male patient was mobile with the skin, was firm, with a spontaneus pain and sensitivity to touch and a growing history form about 5 days ago (Figs. 1a and 1b). There was no other local or general symptoms, no limphadenopathy, no bleeding and no previous trauma. Some balck comedos were observed on the cheeks around the lesion and some scales near the nose. Dermoscopy revealed a 3- mm lesion with homogenous light brown pattern with some brown pigmented globules and black dots and a circular white-yellow pustule at the periphery (Fig. 1c). A presumptive diagnostic of compound nevus with neval folliculitis was made.

Figure 1a: Painful brown lesion on the left cheek.

Figure 1b: Nevus on the left cheek, comedos, scales.
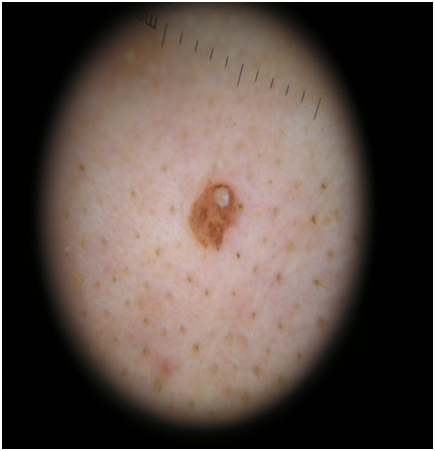
Figure 1c: Neval folliculitis (Dermoscopy 10x).
After a literature review, I wanted to have an answer thees these ions:
1.Is this folliculitis a trauma for the nevus?and if so this trauma is a melanoma inductor?
2.Which type of intradermal nevi gives more frequent the opportunity to appear a subnevic folliculitis-Unna or Miescher nevus?
3.Why this folliculitis affect a nevi?
4.Is it an inflammatory follicullitis or an infectious one?
5.If it is infectious is it a saprophyte germ or is it aquired?
6.You should excise it or you should treat and leave it on the skin?
The bacteriological exam was negative. Follicular rupture, pimple formation, acne or ingrown hairs from plucking can cause rapid apparent growth in a nevus usually accompanied by tenderness and erythema. Topical (fusidic acid) and systemic antibiotics (cefuroxime) were recomended and the surgical removal of the lesion was not considered. When subneval folliculitis is suspected and the nevus fails to settle back within a month conservative excisional biopsy and microscopic examination are indicated.
References:
1. Yus ES, del Cerro M, Simón RS, Herrera M, Rueda M Unna's and Miescher's nevi: two different types of intradermal nevus: hypothesis concerning their histogenesis. Am J Dermatopathol. 2007;29:141-51
2. Sowa J, Kobayashi H, Ishii M, Kimura T. Histopathologic findings in Unna's nevus suggest it is a tardive congenital nevus. Dermatopathol. 2008;30:561-6.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.