|
|
Multiple pigmented clear cell acanthomas associated with squamous cell carcinoma
Ryme Dassouli 1, Zakia Douhi1, Kenza Tahri1, Khaoula Abdellaoui2, Hanane Baybay1, Sara Elloudi1, Laila Tahiri2, Hinde El Fatemi2, Fatima Zahra Mernissi1
1, Zakia Douhi1, Kenza Tahri1, Khaoula Abdellaoui2, Hanane Baybay1, Sara Elloudi1, Laila Tahiri2, Hinde El Fatemi2, Fatima Zahra Mernissi1
1Department of Dermatology, University Hospital Hassan II, Fes, Morocco, 2Department of histopathology, University Hospital Hassan II, Fes, Morocco
Corresponding author: Ryme Dassouli, MD
Submission: 14.12.2021; Acceptance: 18.03.2022
DOI: 10.7241/ourd.2022e.42
Cite this article: Dassouli R, Douhi Z, Tahri K, Abdellaoui K, Baybay H, Elloudi S, Tahiri L, Fatemi HE, Mernissi FZ. Multiple pigmented clear cell acanthomas associated with squamous cell carcinoma. Our Dermatol Online. 2022;13(e):e42.
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
(CCA) is a rare clinical entity characterized by glycogen-rich clear cells with neutrophilic exocytosis [1]. In its multiple form, an association with underlying neoplasia is of concern. Dermoscopy has shown its importance in identifying CCA according to its different stages of maturity. We hilight the role of dermoscopy in the fortuitous discovery of CCAs initially taken as Bowen in a patient with squamous cell carcinoma [2].
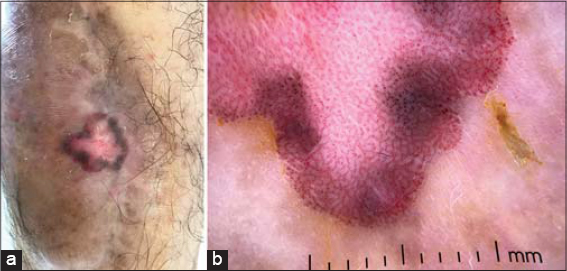
A 65 year old patient, victim of a road accident 5 years ago, with multiple fractures of the legs and history of several episodes of osteomyelitis. He consulted for a plaque on the left foot dating back 5 years, which appeared at the site of the old scar, the size of the tumor was increasing progressively, a biopsy was performed in favor of a squamous cell carcinoma. The dermatological examination revealed an ulcerating tumor on the dorsum of the left foot, 9 cm in length, with a low infiltration. He also presented 4 raised erythematous lesions on the leg, with carcinated and pigmented borders (Fig. 1a). The dermoscopic analysis revealed a vascular pattern made of dotted vessels and linear vessels that took a linear arrangement in the periphery in Indian thread, and further down we noted a pearl necklace arrangement of vessels separated by thick whitish lines realizing a global labyrinthine aspect (Fig. 1b). The lymph node examination was normal. Suspicious right unguinal adenopathies were found in the ultrasound examination. The controlateral location of the adenopathies prompted us to perform a CTAP scan in search of another primary neoplasia. However, the scan did not show any tumor lor deep adenopathy. Anatomopathological examination showed a hyperplastic acanthosis epidermis with elongation and confluence of the epidermal ridges, made of large keratinocytes with pale cytoplasm, associated with an interkeratinocyte inflammatory infiltrate made of neutrophils and eosinophils. The edematous appearance of the dermal papillae was striking, including numerous dilated capillaries. The appearance was in favor of clear cell acanthomas. The attitude was conservative for CCAs and the patient had benefited from an excision of the squamous cell carcinoma with lymph node curage and a close surveillance of the biopsy sites of CCAs.
|
Figure 1: (a) Raised erythematous lesions, roughly oval with carcinated and pigmented borders, located on rights thigh and leg. (b) Dermocopic image showing dotted or glomerular vessels in a serpiginous or pearl-string mesh arrangement. |
CCA is a benign epidermal lesion that often manifests as a single, asymptomatic, erythematous papule or nodule appearing on the extremities. Although its clinical appearance remains nonspecific, CCA has overlapping features with several other lesions, making it difficult to distinguish [3]. Conversely, CCA is known for its characteristic dermoscopic finding of stippled or glomerular vessels in a serpiginous arrangement known as a string of pearls. In more mature forms, the vessels acquire a more coiled appearance in thicker variants, surrounded by whitish cords corresponding to the extent of inflammation responsible for a labyrinthine arrangement [4].
In our case, the clinical presentation associates lesions at different stages of maturation, so that the dermoscopic analysis finds a linear arrangement of the vascular structures in single file in certain places, and a pearl necklace arrangement separated in certain places by large intertwined whitish lines creating a labyrinthine appearance. This appearance is mainly found in the most mature or clinically infiltrated areas.
Furthermore, the etiology of this epithelial proliferation is still unclear. Some authors have proposed that CCA represents a benign epithelial neoplasm, while other recent reports have provided evidence that it may be a pattern of epidermal reaction of inflammatory origin or a paraneoplastic reaction to a neoplasm [5]. In addition, CCA has been described as having malignant degenerative potential [6,7].
In our case, the relationship between multiple CCA and squamous cell carcinoma is unclear. Is it a malignant degeneration of CCA into squamous cell carcinoma, or an installation of CCA due to epidermal proliferation induced by an underlying neoplastic phenomenon, or a response to the systemic inflammatory state conditioned by multiple bone fractures with vicious circles of repetitive bacterial superinfections.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Kiyohara T, Shijimaya T, Miyamoto M, Nagano N, Nakamaru S, Makimura K, et al. Pigmented clear cell acanthoma with a string of pearls pattern on dermoscopy:The first case demonstrating visualization. J Dermatol. 2019;46:e258-9.
2. Iseki K, Negishi M, Nakano M, Togawa Y, Matsue H. Differences in dermoscopic findings between early and mature clear cell acanthoma. J Dermatol. 2020;47:646-50.
3. Tiodorovic-Zivkovic D, Lallas A, Longo C, Moscarella E, Zalaudek I, Argenziano G. Dermoscopy of clear cell acanthoma. J Am Acad Dermatol. 2015;72:S47-9.
4. Lyons G, Chamberlain AJ, Kelly JW. Dermoscopic features of clear cell acanthoma:five new cases and a review of existing published cases. Australas J Dermatol. 2015;56:206-11.
5. Zhang LW, Wang WJ, Li CH, Chen T. The string of pearls pattern in dermoscopy of a chest papule. An Bras Dermatol. 2020;95:392-3.
6. Cunha DG, Kassuga-Roisman LEBP, Silveira LKCB, Macedo FC. Dermoscopic features of clear cell acanthoma. An Bras Dermatol. 2018;93:449-50.
7. Deitermann AM, Fiessinger LA, Miller DD, Jaimes JP. Polarizing-specific white lines in a clear cell acanthoma. JAAD Case Rep. 2020;6:829-31.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-4330-4429
http://orcid.org/0000-0003-3455-3810
http://orcid.org/0000-0002-5942-441X http://orcid.org/0000-0003-4330-4429
http://orcid.org/0000-0003-3455-3810
http://orcid.org/0000-0002-5942-441X
|

Comments are closed.