Subungual acral fibromyxoma: New dermoscopic features
Sanae Sialiti , Asmae Abdelmouttalib, Karima Senouci, Mariame Meziane
, Asmae Abdelmouttalib, Karima Senouci, Mariame Meziane
Department of Dermatology, University Hospital Ibn Sina Rabat, Morocco
Corresponding author: Dr. Sanae Sialiti
Submission: 03.06.2020; Acceptance: 30.12.2020
DOI: 10.7241/ourd.2021e.9
Cite this article: Sialiti S, Abdelmouttalib A, Senouci K, Meziane M. Subungual acral fi bromyxoma: New dermoscopic features. Our Dermatol Online. 2021;12(e):e9.
Citation tools:

Copyright information
© Our Dermatology Online 2021. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
A 34-year-old Moroccan female presented with a painless, firm, slow-growing tumor on the second left toe for the past two years with the involvement of the nail and matrix. A physical examination showed a firm, skin-colored tumor 3 cm in diameter, which had raised and displaced the nail (Fig. 1). Dermoscopic features included a yellowish hyperkeratotic finger-like projection (Fig. 2a), areas with a total white scar-like patch, and linear vessels (Fig. 2b).
 |
Figure 1: Superficial acral fibromyxoma of the second toe. |
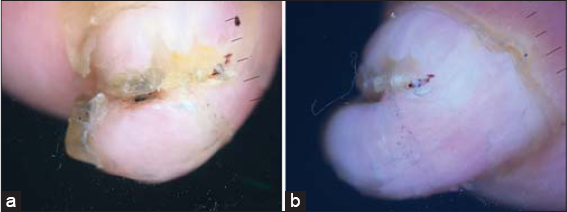 |
Figure 2: (a ans b) Superficial acral fibromyxoma with the following dermoscopic features: a yellowish hyperkeratotic finger-like projection, linear vessels, and a total white scar-like patch. (DermLite DL3, polarized; original magnification: 20×). |
The lesion was surgically removed and a histopathological study confirmed the diagnosis of superficial acral fibromyxoma with fibroblast-like fusiform and stellate cells in a matrix of myxoid material and collagen. An immunohistochemical study of the tumor proved positive for CD34 and CD99, and negative for EMA (Fig. 3).
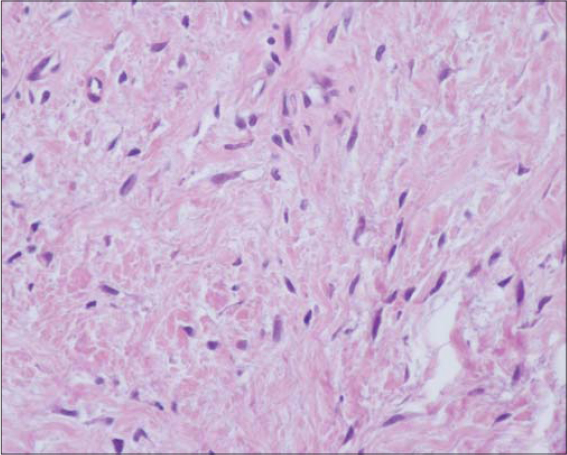 |
Figure 3: Superficial acral fibromyxoma with fibroblast-like fusiform and stellate cells in a matrix of myxoid material and collagen. |
This type of tumor was first described in 2001 and very few cases have since been reported. Superficial acral fibromyxoma classically presents as a pink to flesh-colored nodule located on the subungual or periungual region of the hands or feet. It is typically slow-growing and asymptomatic, which, coupled with its nonspecific clinical appearance, presents a diagnostic dilemma to the dermatologist [1].
Awareness of this rare type of tumor is essential because of the amounts of benign and malignant neoplasms. The diagnosis is established by clinicopathological and immunohistochemical examination. In our case, the dermoscopic examination revealed a yellowish, hyperkeratotic, finger-like projection, a structureless homogeneous white area in the tumor, and linear vessels, which differs from the dermoscopic description reached in a study by Grigore [2].
The standard treatment of subungual acral fibromyxoma is surgery with complete local resection of the tumor. There have been reports of cases treated by partial excision and partial or complete digital amputation. An incomplete tumoral excision may lead to persistent or recurrent cases in up to 20% of the times [2].
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients have given consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Sawaya JL, Khachemoune A. Superficial acral fibromyxoma. Int J Dermatol. 2015;54:499508.
2. Grigore LE, Baican CI, Botar-Jid C, Rogojan L, Letca AF, Ungureanu L, et al. Clinico-pathologic, dermoscopic and ultrasound examination of a rare acral tumour involving the nail – case report and review of the literature. Clujul Med. 2016;89:1604.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.