Squamous cell carcinoma on a Buruli ulcer graft scar: Ivory Coast
Almamy Diabaté 1, Ida Aurélie Lenga Loumingou2, Mienwoley Armel Oussou1, Mutiyu Akanbi Sule3, Irené Gué1, Amon Anderson Stephen Kouabenan1, Bamba Vagamon1
1, Ida Aurélie Lenga Loumingou2, Mienwoley Armel Oussou1, Mutiyu Akanbi Sule3, Irené Gué1, Amon Anderson Stephen Kouabenan1, Bamba Vagamon1
1Department of Dermatology, CHU of Bouaké, Ivory Coast, 2Marein NGouabi University of Brazzaville, Republic of Congo, 3Alassane Ouattara University of Bouaké, Ivory Coast
Citation tools:


Copyright information
© Our Dermatology Online 2023. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
The Buruli ulcer is an infectious necrotizing panniculitis due to Mycobacterium ulcerans, which heals leaving scars. On these scars, squamous cell carcinoma may occur in the long term, even in the case of skin grafting. Herein, we report a case of squamous cell carcinoma occurring on a directed Buruli ulcer scar. A 35-year-old patient with a history of a Buruli ulcer healed with a skin graft in a specialized center for about thirteen years consulted for a cauliflower-like, ulcerating swelling on the left elbow. An examination revealed a large, ulcerating, cauliflower-like swelling. The diagnosis of squamous cell carcinoma was retained, and an amputation was performed without chemotherapy. There was no recurrence after six months of follow-up. After good healing, the Buruli ulcer seemed to present a risk of long-term evolution toward cancer. This observation raises the question of the carcinogenic role of Mycobacterium ulcerans.
Key words: Buruli ulcer; Scar; Squamous cell carcinoma
INTRODUCTION
Buruli ulcer is an infectious necrotizing panniculitis caused by Mycobacterium ulcerans [1]. Currently, the endemic continues to grow and its incidence is increasing dramatically, especially in West African countries such as Ivory Coast. The Buruli ulcer is characterized by its chronic evolution, characterized by extensive skin eruptions complicated by dystrophic, fibrous, and retractile scars [2–5]. On the other hand, directed healing gives considerable scars resistant to traumatic events. On these fibrous scars, squamous cell carcinoma may occur in the long term. In Abidjan, the first case was observed in 2010 [6], then eight cases were observed in 2015 [1], and finally one case in Bouaké in 2019. However, there has been no report on directed scars. Herein, we report a case of squamous cell carcinoma occurring on directed scarring of a Buruli ulcer in a 35-year-old patient without comorbidities.
CASE REPORT
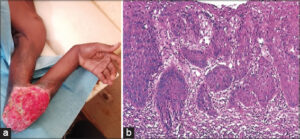
A 35-year-old, HIV-negative patient with a history of a Buruli ulcer healed with a skin graft in a specialized Buruli ulcer management center in Kongouanou (Yamoussoukro) for around thirteen years consulted for an ulcerating swelling on the left elbow present for the past two months. An examination revealed a large swelling, around 12 cm in diameter, ulcerating and bubbling, with a cauliflower-like appearance, bleeding easily on contact, painful, and located on the inner side of the left elbow (Fig. 1a). The peri-lesional skin was normal in appearance. Biology revealed normocytic hypochromic anemia. Histology revealed a proliferation of atypical squamous cells (large hyperchromatic nuclei, numerous mitoses) in invasive lobules, associated with disorders of keratinization. Finally, the tumor stroma was inflammatory (Fig. 1b). An X-ray of the elbow showed bone lysis. The diagnosis of squamous cell carcinoma without metastasis was retained. Amputation was performed without chemotherapy. There was no recurrence after six months of follow-up.
DISCUSSION
The Buruli ulcer is hyperendemic in West and Central Africa: 16,517 cases were recorded from 2006 to 2015, and about five hundred new cases are recorded each year in Côte d’Ivoire, which remains a highly active focus [4]. The epidemiology of the infection responsible for scarring [5,7] explains the young age of our patient and the location of the carcinoma on the limb. No comorbidity, in particular, HIV infection, which is a factor favoring the development of malignant tumors in sub-Saharan Africa, was noted in our observation. The healing of the lesions occurred after several months of treatment. In our report, our patient had highly satisfactory scars after directed healing. The occurrence of cancer in Buruli ulcer scars is known [1,6].
Isolated cases of squamous cell carcinoma have already been described [8,9]. The first Ivorian observation was in 2010 [6]. Since then, eight cases have been recruited by the Abidjan center, which suggests a higher number at the national level since the Abidjan center does not have a monopoly on Buruli ulcer management. All these cases developed on fibrous and retractile scars. If sun exposure is the main risk factor for cutaneous squamous cell carcinoma in fair-skinned people, non-sun factors would be involved in people with pigmented skin. These are mainly chronic leg ulcers (neglected post-traumatic or infectious), HIV infection, discoid lupus, and various chronic scars [10,11]. Carcinomatous degeneration of scars, including scars from old burns, is consistently reported.
There is a lack of epidemiologic studies on this topic in North African and sub-Saharan African countries, where sunlight is high, medical resources are limited, and the risk of repeated scar ulceration becomes higher. The etiology of cancers occurring on scars is not fully understood, although the current hypotheses include proliferation due to chronic inflammation and tissue irritation. In addition, ongoing tissue exposure to toxins and co-carcinogenic factors after injury, as well as poor vascularization of scar tissue, weakens local immune defenses [12–14]. The characteristics of Buruli ulcer scars, which resemble burn scars, may explain why they are particularly prone to carcinomatous degeneration. On the other hand, our patient benefited from directed healing and, thus, a better-quality scar with good vascularization.
Moreover, one may also evoke the chronicity of the wound in this infection or wonder if the mycobacterium itself may not have played a role in carcinogenesis. This observation is, in our opinion, a warning signal. Given the number of people affected by this disease in their childhood or adolescence in Côte d’Ivoire and more generally in sub-Saharan Africa, it is to be feared that there will be a recrudescence of cases in the years to come when these adolescents reach adulthood. To this end, preventive measures should be taken from now on in the countries concerned: the introduction of systematic surveillance of patients “cured” of the Buruli ulcer in order to detect the first signs of carcinomatous degeneration and to sensitize the patients to an early consultation in front of any modification of their scars. This carcinological prevention requires very early management (at a stage without bone involvement or metastasis) of cases to improve the prognosis.
CONCLUSION
After a complete healing, the Buruli ulcer appears to have a long-term risk of progression to cancer. The scars of this condition may be considered precancerous lesions. This observation puts into question the safety of directed healing and the carcinogenic role of Mycobacterium ulcerans.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Kaloga M, Kourouma H-S, DiabatéA, Gbery P, SangaréA ElidjéE-J, et al. Carcinomes épidermoïdes sur cicatrices d’ulcère de Buruli en Afrique de l’Ouest. Ann Dermatol Vénéréol. 2016;143:16-20.
2. Koudoukpo C, Atadokpede F, Salissou L, Assogba F, Akpadjan F, Degboe B, et al. [Clinical evaluation of the deadline of healing of the ulcer of Buruli hurts of diameter lower or equal to 10 centimeters in pobe (Benin)]. Our Dermatol Online. 2016;7:139-44.
3. Saka B, Landoh DE, Kobara B, Djadou KE, Yaya I, YékpléKB, et al. Profil de l’ulcère de Buruli pris en charge au Centre national de reference du Togo:étude de 119 cas. Bull Soc Pathol Exot. 2013;106:326.
4. Ecra E, Yoboue P, Aka B, Gbery P, Sangare A, Kanga K, et al. Les complications de l’ulcère de Buruli:Analyse de 97 cas. Med Afr Noire. 2001;48:4.
5. Kanga JM, Kacou ED, KouaméK, Kassi K, Kaloga M, Yao JK, et al. Lutte contre l’ulcère de Buruli. Expérience de la Côte d’Ivoire. Bull Soc Pathol Exot. 2006;99:348.
6. Kassi K, Kouame K, Allen W, Kouassi LA, Ance W, Kanga JM. Squamous cell carcinoma secondary to Buruli ulcer:A clinical case report in a young girl. Bacteriol Virusol Parazitol Epidemiol. 2010;55:258.
7. Nienhuis WA, Stienstra Y, Thompson WA, Awuah PC, Abass KM, Tuah W, et al. Antimicrobial treatment for early, limited Mycobacterium ulcerans infection:A randomised controlled trial. Lancet. 2010;375:66472.
8. Minutilli E, Orefici G, Pardini M, Giannoni F, Muscardin LM, Massi G, et al. Squamous cell carcinoma secondary to Buruli ulcer. Dermatol Surg. 2007;33:8725.
9. El Hadadi F, Mezni L, Znati K, Meziane M, Ismaili N, Benzekri L, et al. Pyoderma gangrenosum mimicking a Buruli’s ulcer in an HIV-positive patient from Ivory Coast. Our Dermatol Online. 2022;13:158-60.
10. Saka B, Souley Z, KombatéK, Mouhari·Toure A, Akakpo S, Napo Koura G, et al. Les cancers cutanés au Togo:223 observations. Med Trop. 2010;70:16971.
11. Dieng MT, Diop NN, Déme A, Sy TN, Niang 50, Ndiaye B. [Squamous cell carcinoma in black patients:80 cases]. Ann Dermatol Venereol. 2004;131:10557.
12. Ouahbi S, Droussi H, Boukind S, Dlimi M, Elatiqi OK, Elamrani MD, et al. Ulcère de Marjolin:Complication redoutable des séquelles de brûlures. Ann Burns Fire Disasters. 2013;26:199204.
13. Wallingford SC, Olsen CM, Plasmeijer E, Green AC. Skin cancer arising in scars:A systematic review. Dermatol Surg. 2011;37:123944.
14. Almamy D, Koffi KPG, Amon ASK, Irenée G, Boussou RA. A case of squamous cell carcinoma occurring on a scar of Buruli ulcer in Bouake, Ivory Coast. PAMJ. 2019;33:246.
Notes
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.