Pseudoepitheliomatous, keratotic and micaceous balanitis: A case report
Hasna Kerrouch , Hicham Titou, Meryem Khalidi, Rachid Frikh, Naoufal Hjira, Mohammed Boui
, Hicham Titou, Meryem Khalidi, Rachid Frikh, Naoufal Hjira, Mohammed Boui
Dermatology Venerology Department, Military Hospital Instruction Mohammed V, University Mohammed V, Rabat, Morocco
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
Pseudoepitheliomatous, keratotic, and micaceous balanitis (PKMB) is an uncommon premalignant and rare condition occurring over the glans in older men who undergo circumcision late in life [1].
It was first described in 1961 by Lortat-Jacob and Civatte, who described it as locally advancing thick hyperkeratotic plaque on the glans penis [2].
It was previously thought a benign condition, but is now believed to be premalignant [3].
Herein, We report a patient with PKMB who, having declined definitive surgery was managed with cryotherapy and lifelong followup.
A 52 year old circumcised male patient presented at the dermatology departement with a 1 year history of gradually enlarging thick scaly plaque on the glans penis. There was no history of itching, or difficulty in urination. He was an ex-smoker.
Patient was non diabetic and there was no history suggestive of sexually transmitted infections. There was no history of bleeding either spontaneously or following minor trauma. He was not taking any medication. He was treated with antiseptic applications and herbal medicines on various occasions.
Examination revealed a thick scaly plaque on the glans penis measuring about 2 cm by 2 cm (Fig. 1). The plaque was not tender or itchy, and was not obstructing the urethral meatus. The rest of the genitalia were normal.
 |
Figure 1: A Thick scaly plaque on the glans penis. |
There were no other significant skin lesions or palpable inguinal lymphadenopathy. Systemic examination was normal.
The initial differential diagnoses included PKMB, hypertrophic lichen sclerosus (LSc), genital warts, keratoacanthoma, penile intraepithelial neoplasia (PeIN), verrucous carcinoma and frank squamous cell carcinoma (SCC).
Blood counts and blood glucose were within normal limits. Serological tests for human immunodeficiency virus, hepatitis B and syphilis were negative.
Based on these findings, biopsy of the lesion was performed under local anesthesia. Histopathology of the lesion revealed epidermal hyperkeratosis, parakeratosis, acanthosis, and papillomatosis with perivascular mononuclear cell infiltrate in the dermis (Fig. 2). There was no evidence of malignancy or cellular atypia in histopathology.
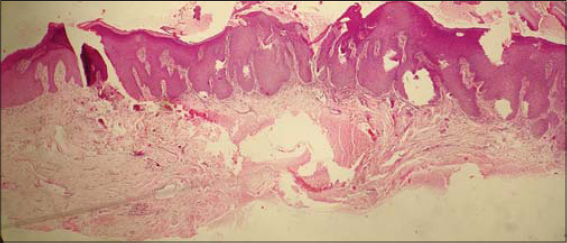 |
Figure 2: Epidermal hyperkeratosis, parakeratosis, acanthosis, and papillomatosis with perivascular mononuclear cell infiltrate in the dermis. |
Based on these clinical and histopathological findings a diagnosis of PKMB was made.
The patient declined definitive surgery and was started on cryotherapy. He had four sessions at monthly intervals to the thicker areas. There was a slight reduction in size of the plaque. He is being regularly followedup.
PKMB is a rare disease that typically occurs on the glans penis in older men [1]. Most patients are over the age of 60 and frequently have been circumcised for phimosis in adult life [1].
The differential diagnosis includes squamous cell carcinoma (SCC), verrucous carcinoma, keratoacanthoma, giant condyloma, penile horn, and erythroplasia of Queyrat [4].
Histopathological examination demonstrates hyperkeratosis, parakeratosis, acanthosis, elongated rete ridges, and mild lower epidermal dysplasia with a nonspecific dermal inflammatory infiltrate of eosinophils and lymphocytes [5].
Krunic et al., theorized that PKMB evolves into four stages; (a) initial plaque stage, (b) late tumor stage, (c) verrucous carcinoma, and (d) transformation to SCC and invasion [6].
Treatment is based on the stage of the lesion. The initial plaque stage can be treated with topical therapy, but advanced stages require a more aggressive approach [7].
Other treatment can be proposed such as x-ray irradiation, shave biopsy plus electrocoagulation, and carbon dioxide laser therapy [6].
Pseudoepitheliomatous, keratotic, and micaceous balanitis is a rare condition and has a characteristic appearance. Long term follow-up is needed for early detection of malignant transformation.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Murthy PS, Kanak K, Raveendra L, Reddy P. Pseudoepitheliomatous, keratotic, and micaceous balanitis. Indian J Dermatol. 2010;55:190-1.
2. Lortat-Jacob E, Civatte J. Balanite pseudo-epitheliomateuse keratosique et micacee. Bull Soc Fr Dermatol Syphiligr. 1961;68:164-72.
3. Beljaards RC, van Dijk E, Hausman R. Is pseudoepitheliomatous, micaceous and keratotic balanitis synonymous with verrucous carcinoma. Br J Dermatol. 1987;117:641-6.
4. Reed SI, Abell E. Pseudoepitheliomatous, keratotic, and micaceous balanitis. Arch Dermatol. 1981;117:4357.
5. Malkud S, Dyavannanavar V. Pseudoepitheliomatous, Keratotic and Micaceous Balanitis:A Case Report. J Clin Diagn Res. 2015;10:WD01-2.
6. Krunic AL, Djerdj K, Starcevic-Bozovic A, Kozomara MM, Martinovic SA, Djokic JH. Pseudoepitheliomatous, keratotic and micaceous balanitis:Case report and review of the literature. Urol Int. 1996;56:125-8.
7. Pai VV, Hanumanthayya K, Naveen KN, Rao R, Dinesh U. Pseudoepitheliomatous, keratotic, and micaceous balanitis presenting as cutaneous horn in an adult male. Indian J Dermatol Venereol Leprol. 2010;76:547-9.
Notes
Source of Support: Nil,
Conflict of Interest: The authors have no conflict of interest to declare.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0001-9290-7627http://orcid.org/0000-0002-2127-3863http://orcid.org/0000-0001-8842-1739 http://orcid.org/0000-0001-9290-7627http://orcid.org/0000-0002-2127-3863http://orcid.org/0000-0001-8842-1739 |

Comments are closed.