A digital myxoid pseudocyst with novel dermoscopic signs
Elga Muralidharan1, Lovleen Kaur 2, Mohita Mahajan1, Bharat Bhushan Mahajan1, Sachdeep Kaur2
2, Mohita Mahajan1, Bharat Bhushan Mahajan1, Sachdeep Kaur2
1Department of Dermatology, Venereology and Leprosy, Government Medical College, Amritsar, Punjab, India, 2Department of Dermatology, Venereology and Leprology, Pt. B.D. Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India
Corresponding author: Dr. Lovleen Kaur, MD
Submission: 21.11.2021; Acceptance: 19.02.2022
DOI: 10.7241/ourd.20223.33
Cite this article: Muralidharan E, Kaur L, Mahajan M, Mahajan BB, Kaur S. A digital myxoid pseudocyst with novel dermoscopic signs. Our Dermatol Online. 2022;13(3):342-343.
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
A 61-year-old female presented to us with a slowly progressive, asymptomatic, localized swelling in the proximal nail fold (PNF) of the left ring finger present for nine months. An examination revealed a discrete, well marginated, skin-colored, firm, non-tender nodule, 8 × 8 mm in size, between the distal interphalangeal (DIP) joint and the PNF of the left ring finger. Besides this, the concomitant nail plate also had longitudinal guttering originating from underneath the PNF and extending until the free edge of the nail plate, corresponding to the possibility of pressure effects of the lesion on the nail matrix (Fig. 1a). Polarized light dermoscopy revealed thick, white, linear structures intermingled with dotted vessels and short, linear, curved, comma-shaped vessels in the center of the lesion (Fig. 2a). High-resolution ultrasonography with power Doppler of the lesion revealed a hypoechoic area without any vascular component (Fig. 2b) and normal appearing interphalangeal joints. Under aseptic precautions, triamcinolone acetonide (TA) at 10 mg/mL was injected intralesionally from its lateral margin until the blanching of the lesion. A transparent, jelly-like material extruded through the entrance of the needle, thus confirming the clinical diagnosis of a digital myxoid pseudocyst (DMP) (Fig. 1b). No recurrence was observed within six months of follow-up (Fig. 1c). A DMP, also called a digital synovial cyst or ganglion cyst, is a benign tumor of the digit. It is not a true cyst as it lacks a cyst wall lined with epithelial cells. It is filled with mucoid materials overproduced by fibroblasts [1]. They arise due to repetitive trauma causing either focal mucinous degeneration of the connective tissue or the leakage of synovial fluid from the DIP joint. Two types of digital mucous cysts are distinguished: the myxomatous, or superficial, type and the ganglion, or deep, type. A DMP may sometimes compress the nail matrix, creating longitudinal depressions in the nail plate, as seen in this case. Nail changes may precede cyst formation by up to six months. Occasionally, the cyst may exert pressure on the nail matrix giving rise to a bluish-red lunula [2]. Salerni et al. described the dermoscopic features of a DMP as bright white areas with a linear, branched, serpentine vascular pattern [3]. Dermoscopy of our case, however, revealed white, linear structures intermingled with dotted vessels and short, linear, curved, comma-shaped vessels. These non-identical dermoscopic patterns could be attributed to the different depth of the DMP in our case to these observed by Salerni et al. The pseudocyst in our case also demonstrated compression effects on the proximal nail matrix indicated by longitudinal guttering in the nail plate, while no such finding was present in the former. In addition, arboriform and polymorphic vascular patterns have also been described. Repetitive puncturing, aspiration, sclerotherapy, and intralesional steroids have been attempted; however, recurrences may develop [4]. Although surgical excision of a DMP with synovectomy shows a lower recurrence rate, it may cause complications such as nail deformities, post-operative pain, and limited post-operative functional use. To conclude, the dermoscopic features of the DMP in the current case may hold an addition to the existing dermoscopic signs, hence aid in the diagnosis of the DMP.
 |
Figure 1: (a) Well-demarcated nodule on the PNF with a concomitant longitudinal groove extending to the free edge of the nail plate; (b) clear, gelatinous substance extruding from the entrance of the needle during triamcinolone acetonide infiltration; (c) the response at twenty weeks after a single injection. |
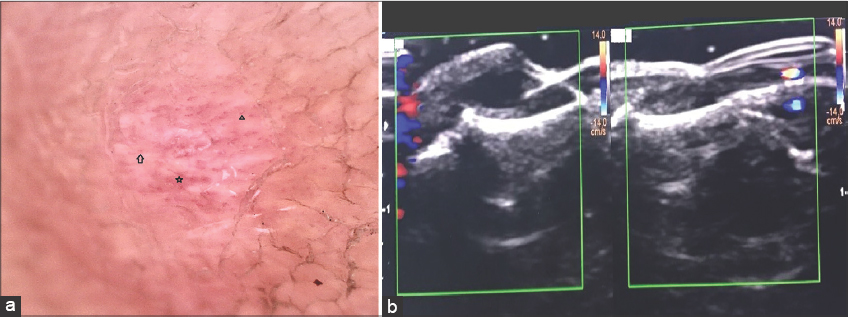 |
Figure 2: (a) Dermoscopy revealing white, linear structures intermingled with dotted vessels (arrow) and short, linear (star) and short, curved or c-shaped vessels (triangle); (b) the hypoechoic area without any vascular component observed on high-resolution ultrasonography with power Doppler of the lesion. |
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Nakamura-Wakatsuki T, Yamamoto T. Cutaneous myxoid cyst on the sclerotic finger in a patient with diffuse systemic sclerosis. Our Dermatol Online. 2013;4:506-7.
2. de Berker D, Goettman S, Baran R. Subungual myxoid cysts:Clinical manifestations and response to therapy. J Am Acad Dermatol. 2002;46:394-8.
3. Salerni G, González R, Alonso C. Dermatoscopic pattern of digital mucous cyst:Report of three cases. Dermatol Pract Concept. 2014;4:65-7.
4. Monteagudo-Sánchez B, Luiña-Méndez L, Mosquera-Fernández A. Dermoscopic features of a digital myxoid cyst. Acta Dermatovenerol Croat. 2019;27:129-30.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-3862-5228 http://orcid.org/0000-0003-3862-5228 |

Comments are closed.