A familial case report of pili torti, pili annulati, and trichorrhexis nodosa showing autosomal dominant inheritance with microscopic findings
Vijeta Prasad, Alpana Mohta , Prasoon Soni, Sumiti Pareek
, Prasoon Soni, Sumiti Pareek
Department of Dermatology, Venereology and Leprology, Sardar Patel Medical College, Bikaner, Rajasthan, India
Corresponding author: Alpana Mohta, MD
Submission: 20.08.2021; Acceptance: 28.04.2022
DOI: 10.7241/ourd.20223.16
Cite this article: Prasad V, Mohta A, Soni P, Pareek S. A familial case report of pili torti, pili annulati, and trichorrhexis nodosa showing autosomal dominant inheritance with microscopic fi ndings. Our Dermatol Online. 2022;13(3):305-307.
Citation tools:

Copyright information
© Our Dermatology Online 2022. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Hair shaft disorders encompass a wide range of hair shaft defects with or without fragility, which could be acquired or inherited genetically. Hair shaft defects may be localized or generalized and are characterized by changes in color, structure, length, and density. Pili torti, also called twisted hair, is a clinical entity in which the hair shaft is flattened and twisted by 180° along its axis. Pili annulati is described as striped hair, showing alternate light and dark bands. Trichorrhexis nodosa is the fracture of the hair shaft. Pili annulati and trichorrhexis nodosa has been reported in a single patient. Herein, we report a familial case of pili torti, pili annulati, and trichorrhexis nodosa with autosomal dominant inheritance.
Key words: Hair shaft disorders; Pili torti; Pili annulati; Trichorrhexis nodosa
INTRODUCTION
Alterations in the hair shaft may be an acquired condition as well as inherited in an autosomal dominant, autosomal recessive, or X-linked manner. A hair shaft defect may be an isolated finding or may be associated with several types of disorders. A complete physical examination along with a microscopic examination is essential for the clinical evaluation and confirmation of the diagnosis [1]. Pili torti is classified as a hair shaft defect with fragility, in which there is flattening and twisting of the hair by 180° [2]. Pili annulati is a hair shaft abnormality characterized by air-filled cavities that, under light microscopy, appear as alternate light and dark bands [3]. Trichorrhexis nodosa is the fracture of the hair shaft appearing as nodes, mostly acquired due to weathering or chemical trauma, yet may rarely be seen with some congenital disorders as well [4].
CASE REPORT
Case 1
A six-year-old female presented with short, lusterless, and fragile blonde hair and complained of her hair not growing in length. On the physical examination of the scalp, diffuse hypotrichosis was present and individual hairs were easily pluckable. On dermoscopy, the hair varied in the hair shaft diameter as well as the color from light brown to some black hairs. The eyebrows and the rest of the body hair were also sparse. The oral mucosa, teeth, and nails were normal. The child had atopic dermatitis and the rest of the skin examination was normal. She showed normal psychomotor development according to her age. Audiometry and ocular examinations were normal. A light microscopic examination showed pili torti, pili annulati, trichorrhexis nodosa, and normal hair (Figs. 1 – 2).
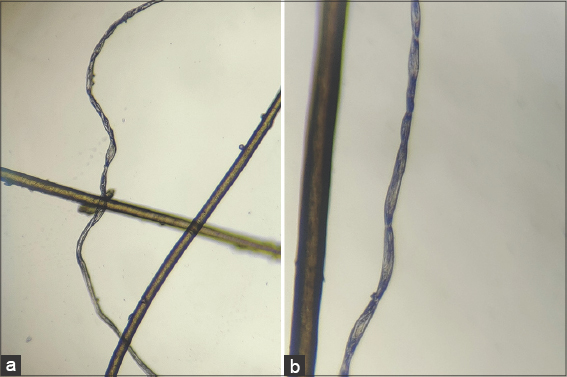 |
Figure 1: (a and b) Microscopic images of pili torti. |
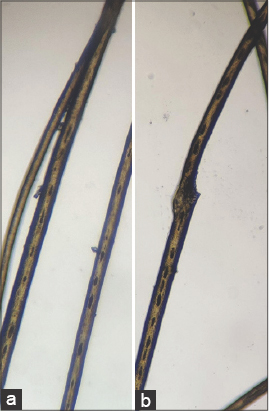 |
Figure 2: (a) Microscopic image of pili annulati. (b) Microscopic image showing pili annulati and trichorrhexis nodosa in the same hair shaft. |
Case 2
A five-year-old brother of case one had similar clinical (Fig. 3a), dermatoscopic, and light microscopic findings. He also had sparse body hair and atopic dermatitis. The rest of the clinical examination was normal, except for the presence of livedo reticularis on the bilateral lower limb (Fig. 3b). ECG and 2D echocardiography were normal.
 |
Figure 3: (a) Short, lusterless, fragile blonde hair with reduced hair density. (b) Livedo reticularis in case two. |
On eliciting a detailed family history, the children’s mother and one of the maternal aunts had similar hair. The rest of the mother’s siblings and family members had no similar findings.
DISCUSSION
Hair shaft disorders are a group of diseases in which there is structural abnormality of the hair with and without fragility. It may be genetic such as monilethrix, pili torti, pili annulati, trichothiodystrophy, genetic trichorrhexis nodosa, wooly hair, etc., as well as acquired such as bubble hair, acquired trichorrhexis nodosa, plica polonica, etc. [2–6]. Pili annulati is a rare hair shaft defect without fragility, in which the hair shows alternate bright and dark bands when observed under reflected light. The bright bands are due to the scattering of light by a cluster of air-filled cavities within the hair shaft. These air-filled cavities in the hair, when viewed under light microscopy, appear as dark [3]. Pili annulati may be seen sporadically or inherited as an autosomal dominant trait. Although pili annulati has been classified as a hair shaft defect without fragility, fragility may be found due to associated trichorrhexis nodosa [7,8]. Trichorrhexis nodosa is the most common among all hair shaft defects and is characterized by hair shaft fracture due to damage to the cuticle and intercellular cement responsible for binding cells together [4]. It may be congenital or acquired. The acquired form is classified as proximal, distal, or circumscribed, occurring due to chemical and physical damage such as blow drying, ironing, and overbrushing. When the fractured part is viewed under light microscopy, separated and splayed-out cortical cells give a thrust paint brush appearance [4]. It may be seen in association with citrullinemia, argininosuccinic aciduria, and tricho-hepato-enteric syndrome. Pili torti is the flattening and twisting of the hair shaft on its own axis by an angle of 180 degrees [2]. It may be inherited or acquired, as in anorexia nervosa and retinoid therapy. It has been reported classically with ectodermal dysplasia and Björnstad syndrome, an autosomal recessive condition with hearing loss [2]. It may also be seen in mitochondrial disorders, urea cycle defects, Menkes disease, and Laron syndrome. A child with pili torti may have abnormal hair from birth or the hair may be normal becoming abnormal during infancy. It may be associated with absent and sparse body hair. There is no specific treatment available for hair shaft disorders. Pili torti may improve in puberty.
CONCLUSION
So far, there have been case reports of trichorrhexis nodosa with pili annulati [7,8]. To the best of our knowledge, ours is the first case of pili torti, pili annulati, and trichorrhexis nodosa in the same individual with autosomal dominant inheritance.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Itin PH, Fistarol SK. Hair shaft abnormalities–Clues to diagnosis and treatment. Dermatology. 2005;211:63-71.
2. Yang JJ, Cade KV, Rezende FC, Pereira JM, Pegas JR. Clinical presentation of pili torti–Case report. An Bras Dermatol. 2015;90:29-31.
3. Akoglu G, Emre S, Metin A, Erbil K M, Akpolat D, Firat A, Hayran M. Pili annulati with fragility:Electron microscopic findings of a case. Int J Trichol. 2012;4:89-92.
4. Kharkar V, Gutte R, Thakkar V, Khopkar U. Trichorrhexis nodosa with nail dystrophy:Diagnosis by dermoscopy. Int J Trichol. 2011;3:105-6.
5. Mancy A. Generalized wooly hair with new associations:A case report. Our Dermatol Online. 2021;12:304-6.
6. Bhat YJ, Shah FY, Keen A. Plica polonica:Trichoscopic findings with a brief literature review. Our Dermatol Online. 2021;12:37-9.
7. Gonzalez AM, Borda LJ, Tosti A. Pili annulati with severe trichorrhexis nodosa:A case report and review of the literature. Skin Appendage Disord. 2019;5:114-6.
8. Donati A, Andriolo AC, Barletta M, Valente N, Romiti R. Pili annulati and trichorrhexis nodosa in the same patient:Cause or coincidence?Skin Appendage Disord. 2015;1:25-7.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0001-7526-2089 http://orcid.org/0000-0001-7526-2089 |

Comments are closed.