Congenital nevus comedonicus complicated by hidradenitis suppurativa-like lesions responding to isotretinoin treatment – A case report form Syria
Heba Fawal 1, Zuheir Al-Shehabi2, Lina Soufi1
1, Zuheir Al-Shehabi2, Lina Soufi1
1Department of Dermatology, National Hospital, Lattakia, Syria, 2Faculty of Medicine, Tishreen Univesity, Lattakia, Syria
Corresponding author: Heba Fawal, MD
How to cite this article: Fawal H, Al-Shehabi Z, Soufi L. Congenital nevus comedonicus complicated by hidradenitis suppurativa-like lesions responding to isotretinoin treatment – A case report form Syria. Our Dermatol Online. 2021;12(3):301-303.
Submission: 02.10.2020; Acceptance: 04.12.2020
DOI: 10.7241/ourd.20213.17
Citation tools:

Copyright information
© Our Dermatology Online 2021. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Nevus comedonicus (NC) is a rare hamartoma of the folliculosebaceous unit clinically characterized by linear lesions composed of numerous dilated follicular openings with keratinous plugs resembling classical comedones, seen mainly on the head and neck. Herein, we present here a case of congenital NC in a young Syrian female distributed along the Blaschko’s lines only on the lower left limb and complicated by multiple hidradenitis suppurativa (HS)-like lesions. The case is unique because of an isolated involvement of a lower limb and a rare association with HS-like lesions, which responded greatly to oral isotretinoin.
Key words: Congenital nevus comedonicus; Hidradenitis suppurativa; Isotretinoin
INTRODUCTION
Nevus comedonicus (NC) is a type of epidermal nevus first described by Kofmann in 1895 [1]. Clinically, it is characterized by linear lesions composed of numerous dilated follicular openings with keratinous plugs resembling classical comedones, seen mainly on the head and neck, followed by the trunk and upper arm. NC associated with HS-like lesions is rare [2]. An isolated involvement of a lower limb, as in our case, has not been reported so far.
CASE REPORT
A fifteen-year-old Syrian female, born of a nonconsanguineous marriage, was referred to our hospital with comedo-like lesions distributed over the lower left limb extending from the lateral aspect of the left buttock up to the end of the left leg along the Blaschko’s lines present since birth, which gradually increased in size and number (Figs. 1a – 1d). After puberty, the patient began to develop recurrent and intolerable painful nodules, abscesses, intercommunicating sinus tracts, and hypertrophic scars involving the buttocks, groin, and popliteal fold. These lesions relapsed or aggravated during hot weather. There was no family history of similar complaints. A physical examination revealed groups of dilated follicular openings filled with keratin distributed over the lower left limb with multiple nodulocystic swellings 2–4 cm in diameter with scarring and fibrous tracts scattered in between. General and systemic examinations were within normal limits, and there was no history suggestive of skeletal, ocular, or other systemic involvement. Routine laboratory investigations, including complete blood count, blood chemistry, and urinalysis were within normal limits. An examination of the lesions with a magnifying glass revealed groups of dilated follicular openings filled with keratin (Fig. 2). Because the patient refused a biopsy, the diagnosis was reached based on clinical manifestations as congenital nevus comedonicus (NC). The HS-like lesions involving the intertriginous areas were taken as being secondary to the NC. The patient was started on oral isotretinoin at a dose of 1 mg/kg/day and intralesional injections of triamcinolone with systemic antibiotics (clavulanic acid with amoxicillin) for ten days. The abscesses were incised and the pus drained. After six months of treatment with isotretinoin, there was a significant improvement in pus discharge and no new lesions developed; in addition, no severe side-effects of the treatment with isotretinoin were observed (Figs. 3 and 4).
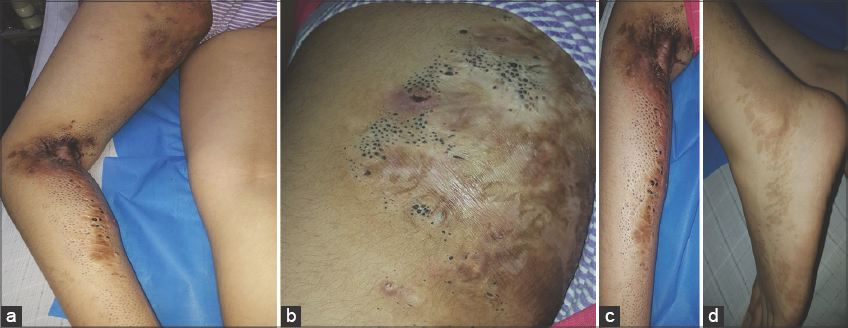 |
Figure 1: (a) Multiple comedo-like lesions and large atrophic pits, resulting in a classic sieve-like appearance present on the lateral aspect of the thigh and leg along the Blaschko’s lines (note the multiple nodules, intercommunicating sinus tracts, and hypertrophic scars). (b) Nevus comedonicus on the left buttock with scars. (c) Nevus comedonicus with nodules, and intercommunicating sinus tracts in the popliteal fold (note the multiple hypertrophic cicatricial contractures). (d) Nevus comedonicus extending onto the left leg and foot. |
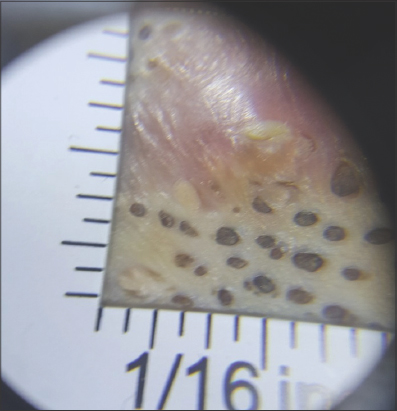 |
Figure 2: Magnification of the nevus revealing groups of dilated follicular openings filled with keratin. |
 |
Figure 3: (a and b) The improvement of the cystic lesions after six months of treatment with oral isotretinoin. |
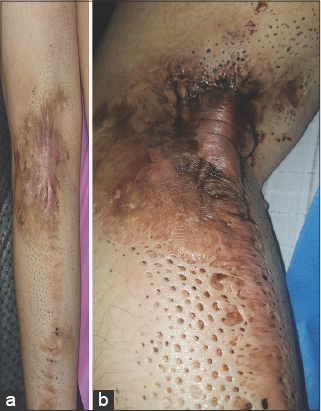 |
Figure 4: (a and b) The improvement of the cystic lesions after six months of treatment with oral isotretinoin. |
DISCUSSION
NC is an uncommon skin abnormality caused by a defect in the development of hair follicles composed of keratin-filled pits. These lesions usually develop at birth or before the age of ten years, but may occur at any time from birth to middle age [3]. Clinically, NC is may be classified as either of two types: type one involves overwhelming numbers of comedones, while type two involves inflammatory changes with late sequelae such as scars, fistulae, and the formation of follicular cysts [4]. Our case was classified as type two. NC may be linear, interrupted, unilateral, bilateral, along the lines of Blaschko, or segmental. The lesions are most commonly located on the face, neck, upper arms, chest, and abdomen [5], and occasionally involve the palms and soles, scalp, female genitalia, and glans penis. The development of HS-like lesions in localized childhood NC is rare. HS is characterized by painful, inflamed nodules, abscesses, intercommunicating sinus tracts, and hypertrophic scarring in apocrine gland-bearing areas, most commonly the axillae and the inguinal and anogenital regions. Follicular plugging occurs congenitally and may be triggered by mechanical stress and hormonal changes, as in puberty [6].
The possible treatment of NC includes excision, dermabrasion, cryotherapy, coagulation, the extraction of the comedones, and the use of topical agents such as retinoic acid, urea, tretinoin, ammonium lactate lotion, tacalcitol, tazarotene, and calcipotriene [7,8]. The therapeutic options for patients with NC complicated by HS include systemic antibiotics, intralesional corticosteroid injections, and oral isotretinoin.
Our patient was treated in all these therapeutic ways and, unexpectedly, showed a significant improvement of the inflammatory lesions and scars. However, there are several reports of NC in which isotretinoin was only minimally effective [9,10].
CONCLUSION
We present a case of congenital nevus comedonicus (NC) in a young Syrian female distributed along the Blaschko’s lines only on the left lower limb and complicated by multiple hidradenitis suppurativa (HS)-like lesions. In contrast to previous reports, our case of NC is exceptional because of an isolated involvement of a lower limb and a rare association with HS-like lesions, which responded greatly to oral isotretinoin.
Consent
The examination of the patient was conducted according to the principles of the Declaration of Helsinki.
The authors certify that they have obtained all appropriate patient consent forms, in which the patients gave their consent for images and other clinical information to be included in the journal. The patients understand that their names and initials will not be published and due effort will be made to conceal their identity, but that anonymity cannot be guaranteed.
REFERENCES
1. Vallabhareddy U, Rao VG, Bikkireddy T, Madala H. Unilateral nevus comedonicus associated with epidermoid cyst. Int J Res Dermatol. 2020;6:560-2.
2. Ravaioli GM, Neri I, Zannetti G, Patrizi A. Congenital nevus comedonicus complicated by a hidradenitis suppurativa-like lesion:Report of a childhood case. Pediatr Dermatol. 2018;35:e298-9.
3. Qian G, Liu T, Zhou C, Zhang Y. Naevus comedonicus syndrome complicated by hidradenitis suppurativa-like lesions responding to acitretin treatment. Acta Derm Venereol. 2015;95:992-3.
4. Bhagwat PV, Tophakhane RS, Rathod RM, Tonita NM, Naidu V. Nevus comedonicus along Blaschko’s lines. Indian J Dermatol Venereol Leprol. 2009;75:330.
5. Solomon LM, Esterly NB. Epidermal and other congenital organoid nevi. Curr Probl Pediatr. 1975;6:1-56.
6. Dufour DN, Bryld LE, Jemec GB. Hidradenitis suppurativa complicating naevus comedonicus:The possible influence of mechanical stress on the development of hidradenitis suppurativa. Dermatology. 2010;220:323-5.
7. Milton GP, DiGiovanna JJ, Peck GL. Treatment of nevus comedonicus with ammonium lactate lotion. J Am Acad Dermatol. 1989;20(2 Pt 2):324-8.
8. Deliduka SB, Kwong PC. Treatment of nevus comedonicus with topical tazarotene and calcipotriene. J Drugs Dermatol. 2004;3:674-6.
9. Peck GL, Yoder FW. Treatment of lamellar ichthyosis and other keratinising dermatoses with an oral synthetic retinoid. Lancet. 1976;2:1172-4.
10. Higgins R, Pink A, Hunger R, Yawalkar N, Navarini AA. Generalized comedones, acne, and hidradenitis suppurativa in a patient with an FGFR2 missense mutation. Front Med (Lausanne). 2017;4:16.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0001-8242-9844 http://orcid.org/0000-0001-8242-9844 |

Comments are closed.