Combined treatment of keloids and scars with Nd:YAG 1064 nm laser and cryotherapy: Report of clinical cases
César Bimbi 1, Piotr Brzeziński2
1, Piotr Brzeziński2
1Dermatology Centro Historico Porto Alegre, Brazil. 2Institute of Biology and Environmental Protection, Department of Cosmetology, Pomeranian Academy, Slupsk, Poland
Corresponding author: Dr. César Bimbi, E-mail: cbimbi@terra.com.br
Submission: 18.06.2019; Acceptance: 22.08.2019
DOI: 10.7241/ourd.20202.8
Cite this article: Bimbi C, Brzeziński P. Combined treatment of keloids and scars with Nd:YAG 1064 nm laser and cryotherapy: Report of clinical cases. Our Dermatol Online. 2020;11(2):149-153.
Citation tools:

Copyright information
© Our Dermatology Online 2020. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Keloids and scars are devastating situations requiring treatment to reduce disfigurement and functional limitations. Therapeutic options should be made on a case-by-case basis. Laser still seems to be an underrated option and has not been so widely used as its efficiency deserves. In this report we investigate the benefits of 1064nm Nd: YAG laser (Genesis, Cutera Inc) applied in non-contact mode on keloids and hypertrophic scars and show how the combination with cryotherapy on elevated parts resulted in obvious clinical improvement of several patients with scars of varied origin, from accidents of transit, work, infections and surgeries. Pulsed light was immensely effective and was also used in the treatment of hyperchromic scars.
Key words: Nd: YAG 1064 nm laser; Cryotherapy; Treatment; Keloids; Hypertrophic scars
INTRODUCTION
Scars are the result of accidents, surgery or some illnesses. Its importance is still underrated and sometimes regarded to be only of cosmetic concern once the patient left the emergency situation. Depending on location scars can also prevent normal movement and can cause pain, dysesthesia and pruritus. Psychological constraints are commom and a heavy weight to the patient to deal with forever.
Keloids are dense fibrous tissue overgrowing beyond the limits of the original wound while hypertrophic scars are more related to thermal or deep dermis injuries and respects the limit of the injury having tendency to diminish. Both are abnormal responses to trauma followed by excessive wound tension inducing fibroblast proliferation and overproduction of dense collagen and glycosaminoglycans.
Presently there is still no single, reliable and effective treatment protocol for keloid and hypertrophic scars. Surgery is indicated for elevated scars, but is contraindicated for flat lesions where high recurrence rates use to happen. Laser therapies have been demonstrated to remodel thickened disorganized tissue accelerating scar maturation leading to good results without complication. Elevated dense hard lesions respond less because thick tissue decreases the efficacy of laser making room for the use of other therapeutic procedures, and we choose cryotherapy which is especially indicated in keloids. Freezing scar tissues induces the differentiation of abnormal keloidal fibroblasts toward a normal phenotype.
CASE REPORTS
Case 1
The patient is a 31-year-old metalworker and he was hit by a car while riding his bicycle to work, an accident that resulted in several hypertrophic and disfiguring scars with keloid raised areas on his face (Fig. 1a). We started sessions of Nd: YAG 1064nm laser Genesis 15 J/cm2, 5-mm spot size. On the more dense and elevated elevated parts of keloids (arrows) we choose to apply cryotherapy in open-spray mode for 30 seconds, with a 3mm margin, every 4 weeks. After a total of 12 treatments, the patient got a good improvement with this combined technique which resulted in flattening of the scar as shown in Figure 1b. The treated scars became more pliable and less hypertrophic (Fig. 1c). Erythema and toughness, itching, and pain also showed improvement and were significantly reduced to nearly normal skin. The patient has been followed now for 5 years since the procedure ended and keloid did not recur.
 |
Figure 1: (a) Hypertrophic disfiguring scars with keloid raised areas. (b) After treatments the patient got a good improvement areas on the face. (c) Skin more pliable. |
Case 2
The patient is a 44-year-old man with linear hypertrophic and erythematous scar from forearm fracture surgery 6 months before (Fig 2a). The scar had not been treated before. After undergoing 5 sessions of 1064 nm Nd: YAG laser treatment (5-mm spot, 15 J/cm2) at monthly interval, the linear raised scar was flattened and erythema reduced (Fig. 2b). Genesis 1064 nm acts collapsing the unnecessary vessels that lead to the red appearance.
 |
Figure 2: (a) Linear erythematous raised scar on forearm since 6 months from forearm fracture surgery. (b) Scar improvement after sessions of laser showing reduced erythema and elevation. |
Case 3
The patient is a 20-year-old male with a solitary keloid papule scar caused by acne (Fig. 3a). After 5 sessions undergoing Nd: YAG laser treatment 20J, 10 ms, 5mm spot, combined with cryotherapy using liquid nitrogen in open-spray mode 15 sec./2mm margin, every 4 weeks, the redness and elevation improved (Fig. 3b) and keloid did not recur after the laser treatment was stopped.
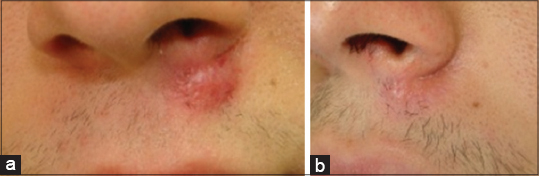 |
Figure 3: (a) Raised keloid papule. (b) 6 months after treatment. |
Case 4
The patient is a 32-year-old woman showing a very common clinical picture consisting of multiple dermal depressions with overlying thinned epidermis due to loss of dermal collagen following type IV acne (Fig. 4a). She had been treated with isotretinoin for 8 months and no more active acne persisted. After 5 sessions undergoing Nd: YAG laser Genesis 18J, 0,8 ms, 8HZ treatment combined with sustained deep dermal heating broadband infrared spectrum of 1100 to 1800nm, 45J to improve facial laxity a more rejuvenated skin were obtained, improving also superficial texture of pitted acne scars (Fig. 4b). Cryotherapy is useless in atrophic scars and was not used in this case.
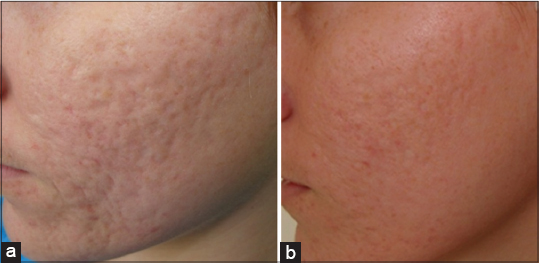 |
Figure 4: (a) Atrophic acne scars following type IV acne. (b) Nd: YAG laser treatment 15 J/cm2 stimulates collagen Production improving the texture of pitted acne scars, enlarged pores, and fine lines. |
Case 5
The patient is a 67-year-old woman showing another very common clinical picture consisting of acne scars combined with loss of dermal collagen due to signs of aging (Fig. 5a). After 5 sessions undergoing Nd: YAG laser 15 J/cm2 treatment combined with sustained deep dermal heating broadband infrared spectrum of 1100 to 1800nm, 45J to improve facial laxity she achieved a very significant improvement (Fig. 5b).
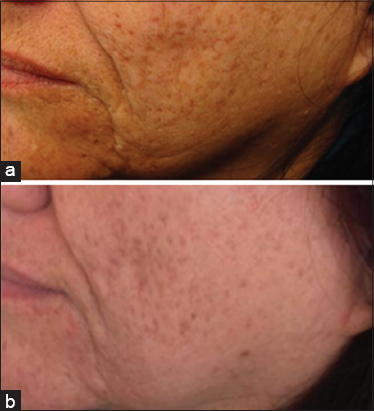 |
Figure 5: (a) Loss of sdermal collagen due to signs of aging. (b) Very significant improvement of facial laxity. |
Case 6
The patient is a 25 years old man who was victim of occupational accident. He had suffered burns with scalding water at work that resulted in hypertrophic scar with blotchy hyperpigmentation (Figs. 6a and 6c). Nd: YAG 1064 laser treatment (10mm spot, 80 J/cm2 40ms) at monthly interval was used. Pulsed light was immensely effective and was also used especially in the treatment of hyperchromic parts of scars. Prowave-770, (handpiece part of Xeo Laser portable platform) 22 J/cm2 has a wavelength range 520nm to 1100nm light which is absorbed by melanin. Pigmented cells are denatured and epidermal melanin first darken and after 3 days tends to diminish. Additionally, we choose to apply cryotherapy in open-spray mode 20 seconds with a 1mm margin, every 4 weeks on the elevated parts. After a total of 10 treatments the patient got a good improvement with this combined technique. This treatment resulted in flattening and whitening of scars with significant reduction of aesthetic changes (Figs. 6b and 6d).
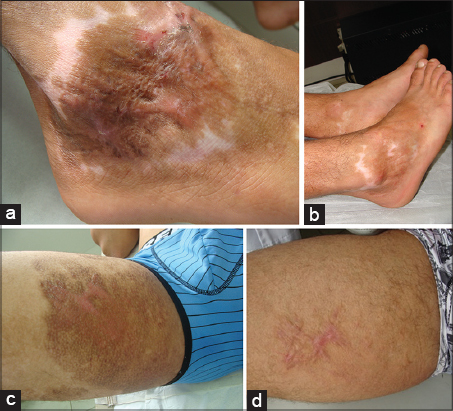 |
Figure 6: (a) Hypertrophic scar with blotchy hyperpigmentation. (b) The patient went a total of 10 treatments. Improvement with flattening, reduced hyperpigmentation. (c) SScars in the inguinal area showing the same characteristics of the previous lesions. (d) Pulsed light sessions were performed to treat pigmentation parts. |
Case 7
The patient is a 30-year-old man with acne keloidalis nuchae (Fig. 7a), a type of folliculitis that form hypertrophic keloid-like scars on the occipital scalp. Short haircuts and close shaving use to be the casual factors. Intralesional triamcinolone acetonide injection cannot be indicated here for active presence of bacteria infection. Active folliculitis was treated with azithromicin and topical clindamicin. Nd: YAG laser treatment (5-mm spot, 15 J/cm2) at monthly interval was applied in every affected area. Prowave 770 ProgramA 22-24 J was necessary for removing infected hairs. Liquid nitrogen was applied and all the area got frozen for 20 seconds, then repeated and so the clinical picture improved (Fig. 7b).
 |
Figure 7: (a) Acne keloidalis nuchae. (b) Inmprovement of hypertrophic keloid-like scars. |
Case 8
The patient is a 18-year-old black girl who works as a model and initially consulted at the clinic complaining of very small and discrete multiple acne scars on his chest that hindered her work. She was advised not to try any procedure for the risk of keloids. She returned months later informing that she had insisted and had been submitted to surgical removal of breast scars with resulted in keloids (Fig. 8). A severe thickening dense irregular and high keloid mass of collagen resulted. YAG Laser did not show any results after 4 sessions and she was referred to a plastic surgeon. Chest keloids growing continuously by the edges have the worst prognosis. Genetics act on keloids and tend to occur on mobile skin that is under high tension. Classical keloid sites are the anterior chest, upper arm and suprapubic region. Tangential excision without suture followed by another method, possibly monthly injections of bleomycin 2m could be recommended.
 |
Figure 8: Irregular keloid mass of collagen. |
DISCUSSION
The report covers 8 cases of pathological cutaneous scars resulting from varied causes such as surgical procedures, acne, infection, trauma, and burns.
Laser scar therapy is said to be a promising and vastly underused tool in the multidisciplinary treatment of traumatic scars [1] deserving a prominent role in future scar treatment paradigms, with the possible inclusion of early intervention for contracture avoidance and assistance with wound healing [2]. The degree of efficiency as well as the various options for complementary treatment for each patient still cannot be determined due to the small number of clinical studies carried out and also for the multiple influences and interferences of parameters such as size, location, and age of the keloid [3].
Laser CO2 is the most popular laser in scars, but being ablative, a substantial downtime will be needed. YAG lasers have the advantage of being well tolerated, with no downtime needed, and no need to avoid work or social activities. Some patients experience mild redness, but it resolves quickly. In fact, both lasers are of great value for scarring. Within only 2 months of receiving the treatment patients already note the keloids become much better than they were before.
Long-pulsed, 1064-nm Nd: YAG Laser Genesis suppress collagen production flattening keloids as demonstrated by Abergel [4] on cultures of keloid fibroblasts. Akaishii [5] from Nippon Medical School Department of Plastic, Reconstructive and Aesthetic Surgery has been using this laser in noncontact mode with low fluence to treat keloids and hypertrophic scars since 2006 with satisfactory results. This is the same equipment that we used on our patients in this report. The efficiency of this Laser decreases with the thickness of the scar, so in thicker parts of keloids, we chose to add cryotherapy. Cryotherapy reduces the activity of fibroblasts and increases the elasticity in keloid tissues [6–8]. The combination of these two techniques showed excellent clinical responses in the patients. We believe even better results might be considered with non-invasive supplementary additional options such as silicone sheeting and interferon retinoic acids neither of which were used during the treatment on our patients. The patients in this report can be divided into groups. Some related to acne scars. While a patient with atrophic scars were treated by Nd: YAG laser treatment 15 J/cm2 which stimulates collagen production improving the texture of pitted acne scars, enlarged pores, and fine lines and deep dermal heating broadband spectrum, the elevated papule of the upper lip in a male patient required additional cryotherapy in open-spray mode and the keloid lost the elevation. A patient of more advanced age achieved a very significant improvement with the combination of Nd: YAG laser 15 J plus sustained deep dermal heating broadband spectrum of 1100 to 1800nm (Titan).
Cutera Xeo Laser portable platform supports a variety of procedures, such as hair removal, skin discoloration treatments, and vascular procedures. Pigmented hypertrophic scars are a difficult condition to treat. Pulsed light has utility in hyperchromic scars. LimeLight handpiece (part of Xeo Laser portable platform) has a wavelength range 520nm to 1100nm light which is absorbed by melanin. Pulsed light sessions were performed to treat pigmentation parts of patient-6. Additionally, we choose to apply cryotherapy. The before-and-after difference is shown on figure6a–b.
The case 1 patient who were victim of road accident with cut in the face went on 1064 nm Nd: YAG laser treatment. It reduces the vascularity decreasing cytokine or growth factor levels and collagen deposition [3]. We started sessions of Nd: YAG 1064nm laser Genesis 15 J/cm2, 5-mm spot size. On the more dense and elevated elevated parts of keloids (arrows) we choose to apply cryotherapy in open-spray mode 30 seconds with a 3mm margin, every 4 weeks. After a total of 12 treatments, the patient got a good improvement with this combined technique which resulted in flattening of the scar and it became more pliable and less hypertrophic, improving itching, pain to nearly normal skin. The skin became dramatically more softened.
The patient of case number 2 showed a surgical raised scar and laser treatment Genesis 1064 nm acted collapsing the unnecessary vessels that lead to the red appearance besides stimulating collagen production. The scar also flattened and of the same normal skin color.
Treatments were well tolerated by all patients and no pain to sever pain was mentioned during the sessions and there was no need for oral analgesic. Crusts occurred as expected only at the points where the cryotherapy was used.
Chest keloids are challenging to treat. Stretching tension as the chest is tends to keloid formation. Acne in the chest or open heart surgery have been frequent causes of keloid formation in the dermatological clinical practice. We have included in this account a dramatic case of chest keloid in a young black model where there has been no improvement with the combined treatment described herein. Unfortunatelly, it was expected for the intense quantity of collagen in the keloid mass. This patient has made the application of nitrogen counterparted due to the risk of residual acromia. In fact, the freezing was not even tempted for this reason. Surgical excision may be the best possible solution and the patient was sent to the plastic surgeon. Surgery alone as a means of chest keloid removal could result in more scars, so it is reserved only for especial situations of elevated lesions by method of tangential without suture excision and followed by complementary treatment [9,10].
It was not the purpose of this paper to use scar scales assesments of the treated scars nor its histological evaluation. Instead, to report cases of patients who got dramatic reduction of the size of their lesions with these two combined therapies.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Waibel J. Miami Dermatology and Laser Institute Florida Keloids and Hypertrophic Scarring:Gaps and Challenges“2014 Vegas Cosmetic Surgery and Aesthetic Dermatology meeting.
2. Anderson RR, Donelan MB, Hivnor C, Greeson E, Ross EV, Shumaker PR, et al. Laser treatment of traumatic scars with an emphasis on ablative fractional laser resurfacing consensus report. JAMA Dermatol. 2014;150:187–93.
3. Mamalis AD, Lev-Tov H, Nguyen DH, Jagdeo JR. Laser and light-based treatment of keloids –a review. J Europ Acad Dermatol Venereol. 2014;28:689-99.
4. Abergel RP, Dwyer RM, Meeker CA, Uitto J, Lask G, Kelly AP. Laser treatment of keloids:A clinical trial and an in vitro study with Nd:YAG laser. Lasers Surg Med. 1984;4:291–5.
5. Akaishi S, Koike S, Dohi T, Kobe K, Hyakusoku H, Ogawa R. Nd:YAG Laser treatment of keloids and hypertrophic scars. Eplasty. 2012;12:e1.
6. Zouboulis CC, Zouridaki E, Rosenberger A, Dalkowski A. Current developments and uses of cryosurgery in the treatment of keloids and hypertrophic scars. Wound Repair Regen. 2002;10:98–102.
7. Dalkowski A, Fimmel S, Beutler C, Zouboulis ChC. Cryotherapy modifies synthetic activity and differentiation of keloidal fibroblasts in vitro. Exp Dermatol. 2003;12:673–81.
8. van Leeuwen MCE, van der Wal MBA, Bulstra AEJ, Galindo-Garre F, Molier J, van Zuijlen PP, et al. Intralesional cryotherapy for treatment of keloid scars:a prospective study. Plast Reconstr Surg. 2015;135:580–9.
9. Sobhy N, El-Shafaei A, Kamal N. Study of fractional ablative laser in surgical and post traumatic scar. Our Dermatol Online. 2012;3:188-95.
10. Park TH, Seo SW, Kim JK, Chang CH. Management of chest keloids. J Cardiothorac Surg. 2011;6:49.
Notes
Source of Support: Nil.
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0002-6396-7767 http://orcid.org/0000-0001-6817-606X http://orcid.org/0000-0002-6396-7767 http://orcid.org/0000-0001-6817-606X |

Comments are closed.