Extramedullary plasmacytomas and prognostic implications in multiple myeloma

1Dermatology Department, Hospital Distrital de Santarém, Santarém, Portugal; 2Clinical Hematology Unit, Hospital Distrital de Santarém, Santarém, Portugal
Corresponding author: Dr. Francisco Gil, E-mail: franciscosgil@gmail.com
Submission: 01.09.2019; Acceptance: 12.11.2019
DOI:10.7241/ourd.20201.23
Cite this article: Gil F, Duarte M. Extramedullary plasmacytomas and prognostic implications in multiple myeloma. Our Dermatol Online. 2020;11(1):84-85.
Citation tools:
BibTex | CSV | RIS | Endnote XML
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Multiple myeloma is a malignant proliferation of monoclonal plasma cells and is often confined to the bone and bone marrow. When the disease affects organs besides the bone or the bone marrow is called extramedullary plasmacytoma [1].
We describe the case of a 68-year-old male, with an IgG lambda multiple myeloma under second-line therapy with bortezomib, thalidomide and dexamethasone after lack of response to first-line treatment, presenting to dermatology department due to the recent development of an erythematous-violaceous nodule of 1,2 cm of diameter on the left flank (Fig. 1), an occipital subcutaneous mass with 5 x 5 cm (Fig. 2) and 4 subcutaneous nodules on the forehead (Fig. 3), between 1,5 and 2 cm of diameter. Lesions were asymptomatic and had grown rapidly in size over weeks. Skin biopsy revealed a dermal and subcutaneous nodular proliferation of immature plasma cells, morphologically and immunohistochemically consistent with cutaneous plasmacytoma. Cranial and maxillofacial computed tomographies were requested, revealing spontaneously dense regular masses at the parietal, right paramedian, frontal and right malar regions, with a lytic infiltrative aspect causing irregularity of the cortical bone and diploe (Fig. 4). The patient died 2 months later from extensive and rapid extra-medullary progression.
 |
Figure 1: Erythematous-violaceous nodule on the left flank. |
 |
Figure 2: Normochromic subcutaneous mass on the occipital region. |
 |
Figure 3: Frontal subcutaneous nodules. |
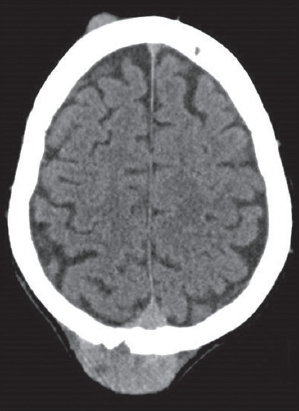 |
Figure 4: Computed tomographic aspect of the extracranial subcutaneous masses. |
Cutaneous plasmacytomas can occur primarily in the skin, without involvement of the bone marrow, or secondarily, from the dissemination of multiple myeloma or plasma cell leukemia [2]. Secondary cutaneous plasmacytomas occur by direct extension from underlying bone lesions or by hematogenic spread. Typically these lesions present as cutaneous or subcutaneous nodules or masses and can be erythematous-violaceous or normochromic [1,2]. There are frequently multiple lesions, of smooth and raised surface, more commonly on the trunk, extremities and face [2]. These lesions occur late in the course of the disease and dictate a poor prognosis, with 50% of the patients dying within 6 months after diagnosis [2,3].
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Yoo J, Jo M, Kim M, Jue M, Park H, Choi K. Cutaneous plasmacytoma:metastasis of multiple myeloma at the fracture site. Ann Dermatol. 2017;29:483–6.
2. Souza D, Muller H, Freitas T, Hungria V, Paes R. Mieloma múltiplo com plasmocitomas cutâneos. An Bras Dermatol. 2004;79:581-5.
3. Bhatnagar A, Verma R, Bhatia J K, Sood A, Das P. Secondary cutaneous plasmacytoma:A bad prognostic marker. J Appl Hematol. 2015;6:172-4.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.