Concomitant erythema induratum of Bazin and papulonecrotic tuberculid: A rare manifestation
Bhusal Priya 1, Joshi Smita1, Adhikari Ram Chandra2
1, Joshi Smita1, Adhikari Ram Chandra2
1Nepal Medical College, Kathmandu, Nepal; 2Department of Pathology, Tribhuvan University Teaching Hospital, Institute of Medicine, Kathmandu, Nepal
Corresponding author: Dr. Bhusal Priya, E-mail: priya.bhusal29@gmail.com
Submission: 16.06.2019; Acceptance: 02.08.2019
DOI: 10.7241/ourd.20201.17
Cite this article: Priya B, Smita J, Chandra AR. Concomitant erythema induratum of Bazin and papulonecrotic tuberculid: A rare manifestation. Our Dermatol Online. 2020;11(1):65-67.
Citation tools:
BibTex | CSV | RIS | Endnote XML
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
The tuberculids represent a group of disorders resulting from hypersensitive immune reactions within the skin due to hematogenous dissemination of Mycobacterium tuberculosis or its antigens from a primary source. Erythema induratum of bazin, papulonecrotic tuberculid and lichen scrofulosorum are classified as true tuberculids. Tuberculids are rare manifestation and simultaneous occurrence of two tuberculids in one patient is even rarer. We report a case of 25 year lady presenting with erythema induratum and papulonecrotic tuberculid simultaneously. Though no source of active infection was found, her lesions were found to be consistent with the diagnosis clinicopathologically and resolved with antitubercular treatment. Concomitant occurrence of two tuberculids in one patient is a rare manifestation and when this has been reported, the commonest combination appeared to be erythema induratum of bazin and papulonecrotic tuberculid, similar to our case, which resolved with antitubercular treatment.
Key words: Erythema induratum of bazin. Papulonecrotic tuberculid. Rare. Simultaneous. Occurrence
INTRODUCTION
The tuberculids represent a group of disorders resulting from hypersensitive immune reactions within the skin due to hematogenous dissemination of Mycobacterium tuberculosis or its antigens from a primary source, occurring in a patient with strong antituberculous cell-mediated immunity. There are three main clinical manifestations of cutaneous tuberculids: lichen scrofulosorum, papulonecrotic tuberculid (PTN) and erythema induratum of Bazin (EI) [1]. The diagnosis of tuberculid may be uncertain when there is an atypical clinical presentation, inconsistent circumstantial evidence, and lack of direct evidence [2]. We report a rare case in which two tuberculids, EI and PTN, occurred simultaneously in the same patient.
CASE REPORT
A 25 years female, previously healthy presented with multiple painful reddish raised solid lesions on both the lower limbs for 1 months. She also developed multiple asymptomatic solid and fluid filled lesions which broke down to form ulcer on upper abdomen, back and both the arms of same duration. She was not suffering from cough, malaise or weight loss but complains of fever which was not documented. She had no past history of tuberculosis (TB), however was living with a family member who suffered from pulmonary tuberculosis.
On cutaneous examination, multiple, tender, erythematous to dusky red, well defined, coin shaped, indurated subcutaneous nodules was present distributed symmetrically over the bilateral lower limb, measuring approximately (1 cm2 – 3 cm2) in size on both calves, shins, left thigh, and right dorsum of foot, some of these had begun to ulcerate (Fig. 1). She also had few vesicles and multiple dusky red papules, some with central necrosis, few scattered and some linearly arranged, discrete, with brownish colored crusts and erythematous border of size 0.5×0.5 cm2 presenton right upper quadrant of abdomen, chest, back and both upper limbs (Fig. 2). There was no evidence of lymphadenopathy. Her systemic examination was unremarkable.
 |
Figure 1: Erythema induratum of bazin. |
 |
Figure 2: Papulonecrotic tuberculid. |
Her routine investigations (hemoglobin, complete blood count, liver function tests, and renal function tests, urine rme) were normal with erythrocyte sedimentation rate of 20 mm/hr. Chest X-ray and abdominal ultrasonography examination were normal. Serology for HIV, HbsAg, anti HCV, VDRL was negative. Examination of tuberculin test site revealed indurated plaque (24 × 24 mm) and multiple erythematous papules at the periphery of the positive tuberculin reaction.
Three biopsy sample were obtained from the characteristic lesion of both eruptions comprising of vesicle, ulcer and nodule. A biopsy specimen of a nodular lesion from the lower leg revealed large area of necrosis involving both septa and lobules with aggregates of histiocytes and necrosis of blood vessel wall (Fig. 3). However, the biopsy specimen of the ulcer and vesicle lesion from the left arm and abdomen respectively showed focal necrosis of dermal collagen with surrounding epithelioid histiocytes, fibrinoid necrosis of vessels with extravasation of red blood cells with perivascular lymphohistiocytic infiltration in the dermis (Fig. 4). These findings were consistent with erythema induratum and papulonecrotic tuberculid, respectively. Acid-fast bacilli were not found in the skin biopsy specimens and PAS stain was negative for fungal element. In view of clinicopathological features, she was started on standard antituberculous regimen consisting of isoniazid, rifampicin, pyrazinamide, and ethambutol for 2 months followed by 4 months of isoniazid and rifampicin. The lesion completely reduced with post inflammatory hyperpigmentation, and atrophy within 4 months of treatment. At the end of 6 month, no recurrence was noted.
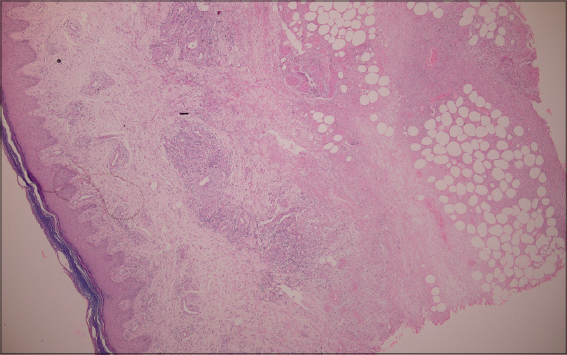 |
Figure 3: Erythema induratum. (H&E; X40 magnification) showing epidermis, dermis and subcutis. The necrosis of subcutaneous lobules and thickening of septa are evident in this magnification. |
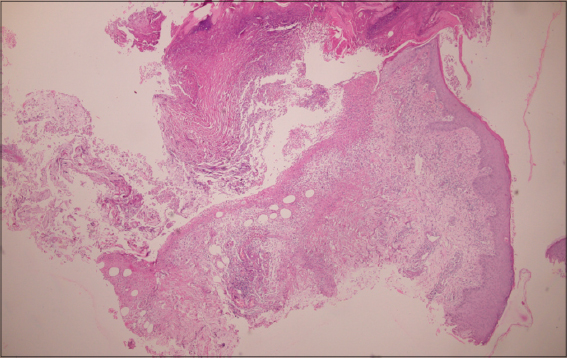 |
Figure 4: Papulonecrotic tuberculid. Low power view (H&E; X40 magnification) showing ulceration and necrosis. |
DISCUSSION
The term tuberculid was coined by Darier in 1896 [3]. Erythema induratum of bazin, papulonecrotic tuberculid and lichen scrofulosorum are generally classified as true tuberculids, i.e., skin manifestations of TB in which no organisms can be demonstrated on acid-fast bacteria (AFB) stain or on culture of the skin lesions [4]. EI have a chronic recurrent course and female preponderance which is presents as persistent nodules or plaques usually sited on the lower third of the calf. The lesion may ulcerate and heal with depressed scar. Histologically a vasculitis affecting small and medium-sized vessels is seen producing a dermal granuloma with epithelioid and giant cells and fat atrophy [5]. PNT occurs as crops of symmetric, small, erythematous, inflammatory papules which have an acral and extensor surface predilection. Lesions may undergo central ulceration and heal spontaneously within weeks, leaving varioliform scars and pigmentation. Microscopically, wedge-shaped area of necrosis is seen with underlying vasculitis and granulomatous infiltrate [4,5].
CONCLUSION
Our patient had both papulonecrotic tuberculid and erythema induratum simultaneously. The clinical and pathological features were entirely consistent with both diagnoses. Her Mantoux test was strongly positive. Although no source of active infection was found this is not unusual. It has been suggested that the failure to detect mycobacteria is a result of rapid destruction of organisms in hypersensitive individuals [6]. The occurrence together of two tuberculids is extremely rare but when this has been reported previously the commonest combination appeared to be PTN and EI as seen in our patient [4].
REFERENCES
1. Asiniwasis R, Dutil MT, Walsh S. Molluscum like papules as a presentation of early papulonecrotic tuberculid in association with nodular tuberculid in male with asymptomatic active pulmonary tuberculosis. J Cut Med Surg. 2015;19:159-62.
2. Oon HH, Chong WS, Oh CC et al. Simultaneous occurrence of papulonecrotic tuberculid and erythema induratum in an Asian Women. Skinmed 2016;14(6);457-459.
3. YH Chuang, TT Kuo, CM Wang, Wang CN, Wong WR, Chan HL. Simultaneous occurrence of papulonecrotic tuberculid and erythema induratum and the identification of Mycobacterium tuberculosis DNA by polymerase chain. Br J Dermatol 1997;137:276-81.
4. Dongre MA, Sanghavi AS, Khopkar SD. Papulonecrotic tuberculid at the site of tuberculin test in a patient with concomitant erythema induratum and papulonecrotic tuberculid. Indian J Dermatol Venereol Leprol. 2013;79:248-50.
5. Mu-Hyoung L. Case of Simulataneous Occurrence of Papulonecrotic tuberculid and erythema induratum. J Dermatol. 2012;40:138-9.
6. Kim GW, Park HJ, Kim HS, Chin HW, Kim SH, Ko HC, et al. Simultaneous Occurrence of papulonecrotic tuberculid and erythema induratum in a patient with pulmonary tuberculosis. Pediatr Dermatol.2013;30:256-9.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
|

Comments are closed.