Guttate psoriasis
Amina Lamouaffaq , Salim Gallouj, Hanane Baybay, Fatima Zahra Mernissi
, Salim Gallouj, Hanane Baybay, Fatima Zahra Mernissi
Department of Dermatology, University Hospital Hassan II, Fez, Morocco
Corresponding author: Dr. Amina Lamouaffaq, E-mail: a.lamouaffaq@gmail.com
Submission: 27.11.2018; Acceptance: 27.01.2019
DOI: 10.7241/ourd.20194.26
Cite this article: Lamouaffaq A, Gallouj S, Baybay H, Mernissi FZ. Guttate psoriasis. Our Dermatol Online. 2019;10(4):400-401.
Citation tools:
BibTex | CSV | RIS | refer/BiblX | Endnote XML
Related Content
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
Sir,
A 13-year-old child, with no pathological history, who presents for 3 years multiple small lesions erythemato-squamous dispersed all over the body, itchy, evolving by push-remission, with worsening winter. Clinical examination revealed multiple erythematous papules, about 5 mm in diameter, with thick whitish scales, at the trunk, back, the elbows and the members (Figs. 1 – 2), with Auspitz sign (Figs. 3a and 3b). The diagnosis of psoriasis gouttata was retained and the child was treated with dermocorticoides and emollient with good improvement after 2 months.
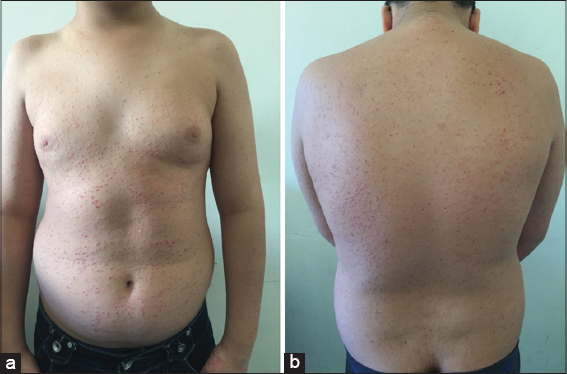 |
Figure 1: (a and b) Multiple erythematous papules, about 5 mm in diameter, with thick whitish scales, at the trunk and back. |
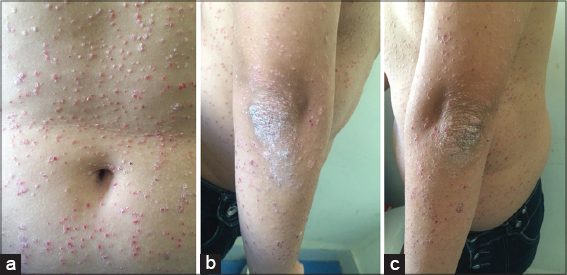 |
Figure 2: (a-c) Multiple erythematous papules, about 5 mm in diameter, with thick whitish scales, at the trunk and elbows. |
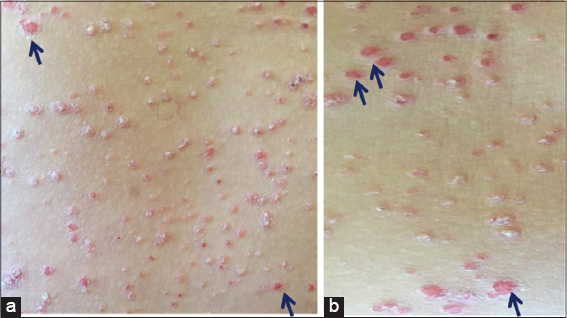 |
Figure 3: (a and b) Auspitz sign (after the scratching of the lesions appear hemorrhagic spots on the erythematous surface). |
Psoriasis is a non-contagious inflammatory disease, predominantly cutaneous, which evolves with exacerbations towards a chronicity. Its prevalence is 1.5-2%. It starts before age 40 in 75% of patients and has 2 peak incidence at 15-25 years and 50-60 years. The etiology is unknown, although it appears to be related to the immune system and environmental factors in people with genetic susceptibility [1,2]. There are several factors that trigger outbreaks of psoriasis, such as physical trauma, bacterial infections (due to the production of superantigens), viral infections, stress and medications [2]. In the case of physical trauma, the phenomenon was recognized by Koebner, in 1872, observed especially in patients who develop the disease at early ages, and has a torpid course. This phenomenon occurs in 20% of cases, and can be seen in other diseases, such as lichen planus, lupus erythematosus or sarcoidosis [3]. The morphology of the lesions is characterized by the presence of homogeneous erythematous plaques covered with scales, Auspitz sign (after the scratching of the lesions appear hemorrhagic spots on the erythematous surface) and Koebner phenomenon [2]. There are different clinical patterns of psoriasis: in plaques (the most frequent), drops or guttate, erythrodermic, pustular and ungueal. Psoriasis guttata predominantly affects children and adolescents, and there are multiple papular lesions with scales of 0.5-1.5 cm, often after a streptococcal infection of the upper respiratory tract, despite the correct antibiotic treatment. Its diagnosis is mainly clinical. The biopsy is performed when the clinical diagnosis offers doubts. In the differential diagnosis should take into account diseases such as pityriasis rosea, lichen planus, secondary syphilis and seborrheic dermatitis. Currently there is no curative treatment, this is aimed at clinical improvement and the decrease in severity. It can be: topical, systemic and phototherapy. The treatment must be individualized according to the severity, the extension, the benefit-risk profile, the patient’s preferences and their response. Emollients will be used for preventive and maintenance treatment; topical treatment in mild forms, avoiding prolonged use of corticosteroids. The combination of vitamin D analogues with corticosteroids is more effective than any of them in monotherapy and is considered the treatment of choice in primary care [1,2].
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Martínez Luya AD, Garcíab RP, Artuñedo AP. Psoriasis guttata. FMC. 2014;21:252-3.
2. Hernández IM, Ruzafa AL, Cavero SC. Psoriasis guttata. FMC. 2007;14:195-8.
3. Ueki H. Koebner phenomenon in lupus erythematosus with special consideration of clinical findings. Autoimmun Rev. 2005;4:219-23.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
Related Content:
| Related Articles |
Search Authors in |
|


|
 http://orcid.org/000-0003-3455-3810 http://orcid.org/000-0003-3455-3810
|
Comments are closed.