Recurrent unilateral linear capillaritis: A very rare variant of pigmented purpuric dermatosis
Fadime Kilinç 1, Akin Aktaş2, Sibel Orhun Yavuz3, Ayşe Akbaş1, Sertaç Şener1
1, Akin Aktaş2, Sibel Orhun Yavuz3, Ayşe Akbaş1, Sertaç Şener1
1Department of Dermatology, Ministry of Health, Ankara City Hospital, Ankara, Turkey; 2Department of Dermatology, Yildirim Beyazit University Medical Faculty, Ankara, Turkey; 3Department of Patology, Ministry of Health, Ankara City Hospital, Ankara, Turkey
Corresponding author: Dr. Fadime Kilinç, E-mail: fykilinc@yahoo.com
Submission: 31.05.2019; Acceptance: 25.07.2019
DOI: 10.7241/ourd.20194.11
Cite this article: Kilinç F, Aktaş A, Yavuz SO, Akbaş A, Şener S. Recurrent unilateral linear capillaritis: A very rare variant of pigmented purpuric dermatosis. Our Dermatol Online. 2019;10(4):361-363.
Citation tools:
BibTex | CSV | RIS | refer/BiblX | Endnote XML
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Pigmented purpuric dermatosis is a disease characterized with localized purpuric lesions. Six different clinical types have been described. There are also unclassified variants including rare granulomatous and unilateral linear capillaritis. Unilateral linear capillaritis is characterized by a very rare, unilateral linear or segmental purpuric macula. A 18-year-old female patient was presented with a linear purpuric and petechial patch and macules on the left arm. Unilateral linear capillaritis is characterized with benign, recurrent purpuric lesions in children and young adolescants that may be presented with spontaneous regression.
Key words: Linear, Pigmented, Unilateral
INTRODUCTION
Pigmented purpuric dermatosis (PPD) is usually characterized with localized purpuric lesions in the lower extremities, and it consists a group of dermatosis with similar histopathological findings caused by an unknown etiology [1–3]. Six different clinical types have been described: Progressive pigmented purpuric dermatosis (Schamberg’s purpura), Purpura annularis telangiectoides (Majocchi purpura), lichen aureus, pigmented purpuric lichenoid dermatosis of Gougerot and Blum, itching purpura and eczematia-like purpura of Doucas and Kapetanakis. There are also unclassified variants including rare granulomatous and unilateral linear capillaritis [2]. Unilateral linear capillaritis (ULC), also known as segmental pigmented purpura or Quadrantik capillaropathy, is characterized by a very rare, unilateral linear or segmental purpuric macula. It is a benign condition presented with spontaneous regression [2,4–6]. As far as we know, 16 cases were reported so far [2]. Since its incidence is rare, our 18-year-old female patient is presented here.
CASE REPORT
A 18-year-old female patient was admitted to our outpatient clinic with complaints of redness on the left arm in November 2017. She had complaints for 3 years and it repeats every 2 months. The lesions were healing in 5-7 days. There were no pain, itching and burning. No family history. She has mitral valve prolapse and she has taken beta blockers (metoprolol) since 2012.
On dermatological examination, she had a linear pigmented rash on the left arm. The eruption consisted of linear purpuric and petechial patch and macules and did not blanch with pressure from a diascope (Figs. 1 and 2). Hemogram and biochemical tests were normal. The clinical diagnosis was felt to be unilateral linear capillaritis. The patient went on to have a 4mm punch biopsy from the left arm.
 |
Figure 1: Linear pigmented purpuric rash on the left arm. |
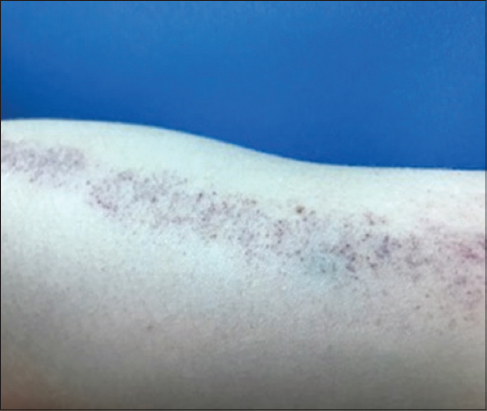 |
Figure 2: A closer view of the lesion. |
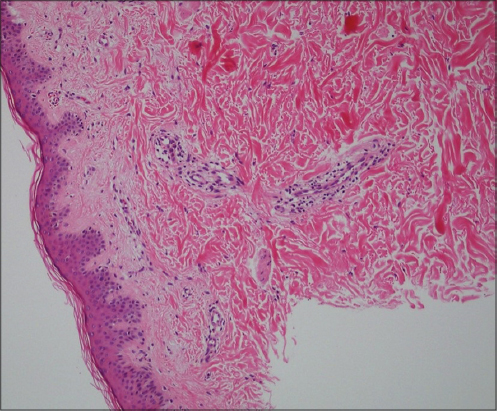 |
Figure 3: Under the epidermis, perivascular lymphocytes and extravascular erythrocytes. |
DISCUSSION
Higgins et al. have identified a female patient with so-called quandrantic capillaropathy [5] in 1990, for the first time. Riordan reported 4 patients with so-called unilateral linear capillaritis in 1992 [7]. PPD is presented usually in middle and older ages, involving lower extremities symmetrical. ULC patients are younger and the lesions disappear spontaneously in about 3 years. The cause of the unilateral and linear involvement is unknown [8].
The suspected etiology include venous hypertension, exercise, capillary fragility, focal infections, alcohol drugs are implicated [9]. Aspirin, carbomal, thiamin, meprobamate, carbamazepine, reserpine, acetaminophen, glipizide, hydralazine are the suspected drugs [8]. The drugs are reported to be the trigger, especially for schamberg disease [1]. Only one of the reported ULC case had been associated with Aspirin [8]. Our patient uses beta-blockers but since she had spontaneous resolution, her condition was not found to be associated with the drugs histopathologically.
So far, 9 (56.25%) of the patients were male and 7 (43.75%) were female. Its incidence is more common in men, but the difference is not significant. The age of the patients range 5 – 48 years. Half of the patients are children. There are two peak ages: 5-15 years (mean 10.12 years) and 23-56 years (mean 35 years). It is usually asymptomatic, Mar reported mild pruritus in two patients [4]. Lower extremity involvement was observed in 11 (68.7%), upper extremity involvement was observed in 4 (25%) and body involvement was observed in 3 (18.7%) patients (1 patient had only body involvement and 2 patients had body involvement with lower extremity involvement). The lesions are usually in segmental configuration, with less linear involvement [2,10]. Since spontaneous regression is observed in a few months or years, generally treatment is not required. Topical steroids, hydroxychloroquine or PUVA may be given if required [8].
The differential diagnoses should include angioma serpiginosum, unilateral naevoid telangiectasia, and lichen aureus firstly [4,11]. Lichen aureus is differentiated by having no band-style lichenoid infiltration on dermis [11].
In conclusion, ULC is a pigmented purpuric dermatosis characterized with benign, recurrent purpuric lesions in children and young adolescants that may be presented with spontaneous regression mostly involving lower extremities with segmental or linear lesions.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Kim DH, Seo SH, Ahn HH, Kye YC, Choi JE. Characteristics and Clinical Manifestations of Pigmented Purpuric Dermatosis. Ann Dermatol. 2015;27:404-10.
2. Elshimy N, Walker B. Unilateral linear capillaritis:A case and summary of the literature 25 years on from its original description. Clin Case Rep Rev. 2017;3:1-3.
3. Aghaei S, Hooshmand F. Unilateral pigmented purpuric dermatosis in an adult patient. Am J Case Rep. 2011;12:181-3.
4. Mar A, Fergin P, Hogan P. Unilateral pigmented purpuric eruption. Australas J Dermatol 1999;40:211-4.
5. Higgins EM, Cox NH. A case of quadrantic capillaropathy. Dermatologica. 1990;180:93-5.
6. Pock L, Capkova S. Segmental Pigmented Purpura. Paediatr Dermatol 2002;19:517-9.
7. Riordan CA, Darley C, Markey AC, Murphy G, Wilkinson JD. Unilateral linear capillaritis. Clin Exp Dermatol. 1992;17:182-5.
8. Taketuchi Y, Chinen T, Ichikawa Y, Ito M. Two cases of unilateral pigmented purpuric dermatosis. J Dermatol 2001;28:493-498.
9. Ozkaya DB, Emiroglu N, Su O, Cengiz FP, Bahali AG, Yildiz P, et al. Dermatoscopic findings of pigmented purpuric dermatosis. An Bras Dermatol. 2016;91:584-7.
10. Abdullah L, Abbas O. Dermacase. Can you identify this condition?Unilateral linear capillaritis. Can Fam Physcian. 2011;57:563.
11. Yüksek J, Sezer E. Pigmente Purpurik Dermatozlar. Türkiye Klinikleri J Dermatol 2008;18:223-7.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0001-9137-2675 http://orcid.org/0000-0001-9137-2675 |

Comments are closed.