Facial granulomatous periorificial dermatitis in a Tunisian child
Anissa Zaouak1, Leila Bouhajja 1, Selima Ben Jannet1, Olfa Khayat2, Houda Hammami1, Samy Fenniche1
1, Selima Ben Jannet1, Olfa Khayat2, Houda Hammami1, Samy Fenniche1
1Department of Dermatology, Habib Thameur Hospital, Tunis, Tunisia; 2Department of Pathology, Habib Thameur Hospital, Tunis, Tunisia
Corresponding author: Dr. Leila Bouhajja, E-mail: bouhaja.leila@gmail.com
Submission: 25.07.2018; Acceptance: 29.11.2018
DOI:10.7241/ourd.20192.19
Cite this article: Zaouak A, Bouhajja L, Jannet SB, Khayat O, Hammami H, Fenniche S. Facial granulomatous periorifi cial dermatitis in a Tunisian child. Our Dermatol Online. 2018;10(2):181-183.
Citation tools:
BibTex | CSV | RIS | refer/BiblX | Endnote XML | Wikipedia Citation Templates
Copyright information
© Our Dermatology Online 2019. No commercial re-use. See rights and permissions. Published by Our Dermatology Online.
ABSTRACT
Childhood granulomatous periorificial dermatitis(CGPD) is a facial rash, affecting the periorificial area in children. We present the case of 7-year-old child, presented with an asymptomatic papular eruption on the face since one year. On physical examination he had numerous monomorphic erythematous papules ranging from 1 to 3 mm in diameter clustered around his perioral region predominantly with sparse papules on his periocular and perinasal regions. A skin biopsy of a perioral papule was performed showing a dense granulomatous infiltrate located around the hair follicles in the deep and superficial dermis composed of epithelioid cells, histiocytes and lymphocytes without caseation necrosis.The patient was treated with erythromycin 500 mg with emollients and his papular eruption resolved. After one year of follow-up, there was no relapse.
Key words: Dermatitis, Child, Granuloma
INTRODUCTION
Childhood granulomatous periorificial dermatitis (CGPD) is a granulomatous skin disease characterized by yellowish brown papules affecting perioral, perinasal and periocular areas. It was first described by Ginotti et al in 1970 in five children [1].It affects mainly black children, but there are cases involving Caucasian patients[2]. The etiology is controversial butthe use of topical medication can be responsible.
CASE REPORT
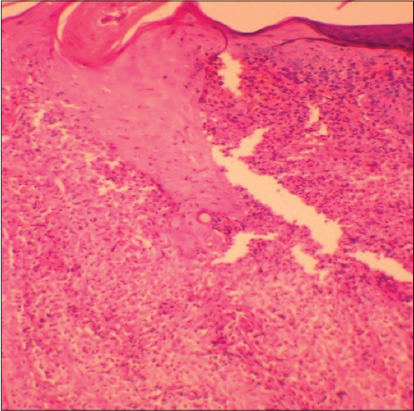
A 7-year-old child presented with an asymptomatic papular eruption on the face since one year. He had no personal or family history of acne, asthma, contact dermatitis or food allergies. Initially he was treated with betamethasone dipropionate 0.05% cream, twice daily on his facial eruption for 3 months by his pediatrician with a worsening of his skin condition. On physical examination, he had numerous monomorphic erythematous papules ranging from 1 to 3 mm in diameter clustered around his perioral region predominantly with sparse papules on his periocular and perinasal regions (Fig.1). The rest of his cutaneous examination was normal. A skin biopsy of a perioral papule was performed showing a dense granulomatous infiltrate located around the hair follicles in the deep and superficial dermis composed of epithelioid cells, histiocytes and lymphocytes. There was no caseation necrosis (Fig.2). The special staining for fungi and mycobacteria were negative. Immediate discontinuation of topical corticosteroids was performed. The patient was treated with erythromycin 500 mg four times a day for 2 months along with emollients. His papular eruption resolved without sequelae and after one year of follow-up, there was no relapse.

DISCUSSION
Childhood granulomatous periorificial dermatitis (CGPD) is a granulomatous disease characterized by monomorphic small papular eruption with a periorificial distribution predominantly in the perioral region. It was first described by Ginotti et al in 1970 in five children [1]. It usually presents as asymptomatic flesh-colored, yellow-brown monomorphic with a periorificial distribution as in our patient with small papules affecting the perioral, periorbital and perinasal folds. Histopathologic examination is important to distinguish this entity from the other cutaneous granulomatosis and shows usually perifollicular epithelioid granulomas without a central caseation necrosis associated to a moderate inflammatory infiltrate located in the dermis and around the vessels. The age range is between 3 and 12 years. It occurs more commonly in dark skinned patients originating from Africa but Caucasian children could also be affected [2]. CGPD is a controversial disease. Its etiology remains unclear. Some authors consider that it could belong to the large spectrum of granulomatous rosacea in children; others consider that it is a distinct entity with a particular clinical behavior. Differential diagnosis may include granulomatous rosacea, cutaneous sarcoidosis, perioral dermatitis, lupus miliaris disseminates facei, perioral contact dermatitis and tinea incognito. Granulomatous rosacea could also be mistaken with CGPD featuring almost the same clinical and histological findings but it is uncommon in children [2–5]. Cutaneous sarcoidosis is uncommon in children, it could mimic CGPD but in sarcoidosis multinucleated giant cells are uncommon.CGPD is a self-limited disease but may be exacerbated by the application of topical steroids. For the treatment, the first step is to convince the parents to an immediate discontinuation of the topical corticosteroids. The second step is to reassure the patient and the parents that it is a benign and self-limited condition that resolves without leaving cutaneous scars. Treatment with oral tetracycline, metronidazole and erythromycin seem to be the most effective. Other treatment alternatives are represented by topical erythromycin, topical metronidazole, topical tacrolimus or azelaic acid cream which could also be useful. Combining oral antibiotics and topical tacrolimus could also be an effective treatment in some patients [6].
CONCLUSION
CGPD is a distinct entity with a self-limited evolution which should be treated with a safe treatment with low side effects. Dermatologists should be aware of this dermatitis since it could affect Caucasian children and could be easily mistaken with the other acneiform eruptions.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Gianotti F, Ermacora E, Benelli MG, Caputo R. Perioral dermatitis in children and adults. G Ital Dermatol Minerva Dermatol. 1971;46:132.
2. Hatanaka M, Kanekura T. Case of childhood granulomatous peiorificial dermatitis. J Dermatol. 2018;45:e256-7.
3. Tiengo A, Barros HR, Carvalho DB, Oliveira GM, Romiti N. Case for diagnosis:childhood granulomatous periorificial dermatitis. An Bras Dermatol. 2013;88:660-2.
4. Dessinioti C, Antoniou C, Katsambas A. Acneiform eruptions. Clin Dermatol. 2014;32:24-34.
5. Lucas CR, Korman NJ, Gilliam AC. Granulomatous periorificial dermatitis:a variant of granulomatous rosacea in children?. J Cutan Med Surg 2009;13:115-18.
6. Hussain W, Daly BM. Granulomatous periorifical dermatitis in an 11-year-old boy:dramatic response to tacrolimus. J Eur Acad Dermatol Venereol.2007;21:137-39.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Request permissions
If you wish to reuse any or all of this article please use the e-mail (brzezoo77@yahoo.com) to contact with publisher.
| Related Articles | Search Authors in |
|
|
 http://orcid.org/0000-0003-2062-2256 http://orcid.org/0000-0003-2062-2256
|

Comments are closed.