|
Get Citation
|
|
|
Urso B, Updyke KM, Solomon JA. Systemic Lupus Erythematosus and the broken dental tool. Our Dermatol Online. 2018;9(1):99-100. |
|
|
Download citation file:
|
Systemic Lupus Erythematosus and the broken dental tool
Brittany Urso1, Katelyn M. Updyke1, James A. Solomon1,2,3
1University of Central Florida College of Medicine, Orlando Florida, USA; 2University of Illinois College of Medicine, Urbana Illinois, USA; 3Ameriderm Research, Ormond Beach Florida, USA
Corresponding author: Brittany Urso, E-mail: Brittany.Urso@knights.ucf.edu
Submission: 30.06.2017; Acceptance: 31.08.2017
DOI: 10.7241/ourd.20181.32
Sir,
Systemic Lupus Erythematosus (SLE) is an autoimmune condition which can be exacerbated by many factors, many of which are unknown. While flares can be controlled with medications, we often are unsure of their cause which makes disease maintenance difficult. It is possible that investigation of a patient’s habits, lifestyle, and diet may provide clues which make disease maintenance, and even remission, possible.
We present a 40-year-old female with a medical history of Systemic Lupus Erythematosus (SLE) associated with contact allergies to nickel, and drug reactions to penicillin, tetracycline, clindamycin, erythromycin, and sulfa. Her first SLE episode occurred following a weekend at a tomato harvest and subsequent episodes followed upper respiratory tract symptoms treated with antibiotics. These episodes resolved spontaneously. A dentist breaking a stainless steel tool, lodging the tip within her tooth, precipitated 2 years of chronic fatigue, joint pains, butterfly rash, peripheral edema, irritable bowel, and general malaise. Her ANA titer was > 1:640 and homogeneous suggesting a drug eruption.
On physical exam, the patient had a butterfly rash and urticarial papules and plaques on her trunk and extremities in a distribution corresponding to areas in contact with metal.
Detailed history of her first SLE episodes were associated with ingesting dozens of tomatoes as well as with taking aspirin with antibiotics. To investigate her allergies, a lymphocytic activation assay was performed under laminal flow hoods, using RPMI media without bovine serum, penicillin or streptomycin. The assay revealed lymphocyte activation to 10-9-10-18 molar to penicillin, salicylates, nickel, cobalt, chrome, and sulfonamide. Additionally, the reaction to salicylates was at 10-9 molar but was 10-18 molar to Bayer Aspirin™ tablet; (n.b.: the tablet combines salicylates with metal fillers).
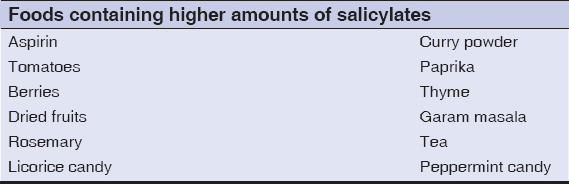
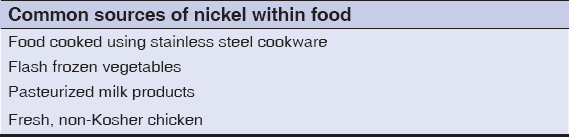
The patient noted significant improvement with dietary restriction of salicylate and nickel containing foods, including tomatoes, as well as avoidance of nickel containing cookware, which not only includes base metal cookware but also stainless steel (Table 1 and 2) [1,2]. Photosensitivity resolved when she avoided food sources of psoralens. Additionally, removal of the dental tool fragment and metal restorations (multiple stainless steel root canal crowns) was associated with complete remission. As result, through careful analysis of the patient’s habits, lifestyle, and diet, we were able to determine and control triggers, such as salicylates, nickel, and drugs which induce photosensitivity, which precipitated her SLE flare.
REFERENCES
1. Swain AR, Dutton SP, Truswell AS. Salicylates in foods. J Am Diet Assoc. 1985;85:950-60.
2. Kamerud KL, Hobbie KA, Anderson KA. Stainless steel leaches nickel and chromium into foods during cooking. J Agric Food Chem. 2013;61:9495-501.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.