|
Get Citation
|
|
|
Arif T, Amin SS, Raj D. Pilomatricoma of the eyelid. Our Dermatol Online. 2017;9(1):73-74. |
|
|
Download citation file:
|
Pilomatricoma of the eyelid
Tasleem Arif, Syed Suhail Amin, Dinesh Raj
Department of Dermatology, STDs and Leprosy, Jawaharlal Nehru Medical College (JNMC), Aligarh Muslim University (AMU), Aligarh, India
Corresponding author: Dr. Tasleem Arif, E-mail: dr_tasleem_arif@yahoo.com
Submission: 28.05.2017; Acceptance: 20.08.2017
DOI: 10.7241/ourd.20181.21
ABSTRACT
Pilomatricoma is an uncommon benign tumor considered to be harmatoma of hair matrix. Here we present a case of 27 year old male patient who had solitary swelling over the right upper eyelid. On the basis of clinical and histopathological background, the diagnosis of pilomatricoma was made.
Key words: Hair matrix; Hamartoma; Pilomatricoma
INTRODUCTION
Pilomatricoma was first described by Albert Hippolyte Malherbe and J. Chenantais as calcifying epithelioma in 1880 A.D [1]. Later on, in 1949 Lever and Griesemer suggested the hair matrix cells to be the origin of the tumor and finally in 1961 Forbis and Helwig proposed the currently accepted name “pilomatricoma” [2,3].
Clinically, the lesion appears as a slowly enlarging, irregularly shaped, rock hard, nodular, non tender mass freely movable over the subcutaneous tissue. The skin usually has reddish to blue discoloration due to dilated blood vessels and chalky white nodules may be seen through the skin. There is typically no history of inflammation or trauma [4]. In this article we present a case of pilomatricoma involving the eyelid.
CASE REPORT
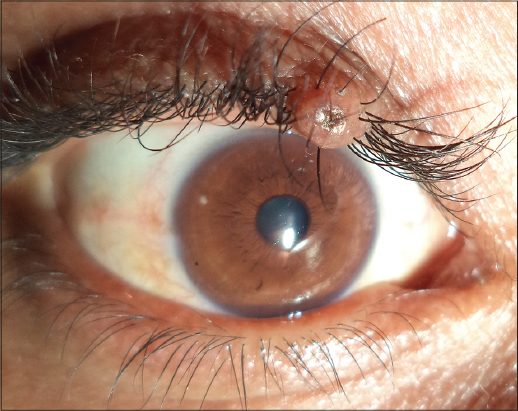
A 27 years old male presented to the hospital with a small painless nodular lesion in the right upper eyelid for 5 years. The history of the patient revealed no pain, previous inflammation or trauma. On examination, a small, round, non-tender, rock hard, nodule was present on right upper eyelid (Figs. 1 and 2). There was hair shaft emanating from the summit of the nodule. It had normal skin color, but chalky white nodules could be seen through the healthy appearing skin. The patient was referred to ophthalmology department where the lesion was excised and sent for histopathological examination which confirmed the diagnosis of pilomatricoma showing a biphasic population composed of basaloid germinative cells and eosinophil shadow cells with a few foci of dystrophic calcification.

DISCUSSION
Pilomatricoma is an ectodermic tumour originating from pluripotential precursors of hair matrix cells. It can present at any age. It demonstrates a bimodal peak presentation during 1st and 6th decades of life, about 40% of cases occur in patients younger than 10 years of age and 60% of cases occur within the first two decades of life. Its more common in females than in males [5]. Clinically, it manifests as asymptomatic, benign solitary, soft and friable to hard nodule measuring 0.5 cm to 5.0 cm. It is subcutaneous slow growing tumor which may or may not be attached to the skin and mobile over underlying structures. It may also present as multiple and nodular pattern in 2% – 10% of the cases. An activation of β catenin gene CTNNBI mutation may be the cause for development of familial pilomatricoma [6]. Multiple and familial pilomatricomas are associated with Steinert’s myotonic dystrophy, Gardner Syndrome, Turner Syndrome and Trisomy 9 [7]. Among lesions that need to be differentiated from a pilomatricoma include epidermal inclusion cyst, sebaceous adenoma, dermoid cyst, epidermoid cyst and vascular tumors.
Histologically, pilomatricoma is characterized by a mass made up by basaloid cells in periphery, ghost cells in central part and calcification and sometimes ossification. The ghost cells represent necrotic areas of previously vital basaloid cells. The calcification and ossification areas appear progressively in necrotic areas. Ghost cells are pathognomic of pilomatricoma[8].
Presenting age of 27 years, eyelid affliction, male sex and absence of any predisposing factors like trauma make our case an uncommon presentation of pilomatricoma and hence reported.
REFERENCES
1. Malherbe, A. and Chenantais, J. Note Sur L’epitheliome calcifie des glades sebacees. Programme Med. 1888;8:826-8.
2. Lever WF, Griesemer RD. Calcifying epithelioma of Malherbe;report of 15 cases, with comments on its differentiation from calcified epidermal cyst and on its histogenesis. Arch Derm Syphilol. 1949;59:506-18.
3. Forbis R Jr, Helwig EB. Pilomatrixoma (calcifyng epithelioma) Arch Dermatol. 1961;83:606-18.
4. Abalo-Lojo JM, Cameselle-Teijeiro J, Gonzalez F. Pilomatrixoma:late onset in two periocular cases. Ophthal Plast Reconstr Surg. 2008;24:60-2.
5. Taaffe A, Wyatt EH, Bury HP. Pilomatrixoma (Malherbe):A clinical and histo pathologic survey of 78 cases. Int. J Dermatol. 1988;27:477-80.
6. Chan, E.F., Gat, U., Mc Niff, J.M. and Fuchus, E. A Common Human Skin Tumor Is Caused by Activating Mutation of β-Catenin. Nature Genetics, 1999;21:410-13.
7. Aslan G, Erdogan B, Akoz T, Gorgu M, Seckin S, Terzioglu A. Multiple occurrence of pilomatrixoma. Plast Reconstr Surg Sept. 1996;98:510-3.
8. Passi N, Chawla U, Jyoti, Khurana AK. Pilomatrixoma of eyelid in a middle aged. Nepal J Ophthalmol. 2011;3:88-90.
Notes
Source of Support: Nil
Conflict of Interest: None declared.
Comments are closed.