Dermatology Eponyms – sign – Lexicon (P). Part 2
Piotr Brzezinski1,2, Masaru Tanaka3, Husein Husein-ElAhmed4, Marco Castori5, Fatou Barro/Traoré6, Satish Kashiram Punshi7, Anca Chiriac8,9
Department of Dermatology, 6th Military Support Unit, Ustka, Poland, 2Institute of Biology and Environmental Protection, Department of Cosmetology, Pomeranian Academy, Slupsk, Poland, 3Department of Dermatology, Tokyo Women’s Medical University Medical Center East, Tokyo, Japan, 4Department of Dermatology, San Cecilio University Hospital, Granada, Spain, 5Medical Genetics, Department of Experimental Medicine, Sapienza – University of Rome, San Camillo-Forlanini Hospital, Rome, Italy, 6Department of Dermatology-Venerology, Yalgado Ouédraogo Teaching Hospital Center (CHU-YO), Ouagadougou, Burkina Faso, 7Consultant in Skin Dieseases, VD, Leprosy & Leucoderma, Rajkamal Chowk, Amravati – 444 601, India, 8Department of Dermatology, Nicolina Medical Center, Iasi, Romania, 9Department of Dermato-Physiology, Apollonia University Iasi, Strada Muzicii nr 2, Iasi-700399, Romania
ABSTRACT
Eponyms are used almost daily in the clinical practice of dermatology. And yet, information about the person behind the eponyms is difficult to find. Indeed, who is? What is this person’s nationality? Is this person alive or dead? How can one find the paper in which this person first described the disease? Eponyms are used to describe not only disease, but also clinical signs, surgical procedures, staining techniques, pharmacological formulations, and even pieces of equipment. In this article we present the symptoms starting with (P) and other. The symptoms and their synonyms, and those who have described this symptom or phenomenon.
Key words: Eponyms; Skin diseases; Sign; Phenomenon
Port-Light Nose sign
Rhinophyma as a progressive, disfiguring disease of the nose, is considered the final stage of acne rosacea [1]. Also called bottle nose (Fig. 1).

Possum Boil Sign
Leptospirosis infection [2]. Also known as Opossum and Skunk sign.
Pot Belly Sign
A classic presentation of pellagra (Figs 2a and 2b) [3–5].

Practolol Sign
Hyperkeratosis of the feet and palms. Associated with carcinoma of the oesophagus and psoriasis [6]. Even though it is a syndrome of low incidence, hyperkeratosis or tylosis palmoplantaris is widely related with the onset of squamous cell carcinoma of the esophagus. Such correlation receives the name Howel-Evans and has a family penetrance close to 100%.
Prayer Sign
1. It is described in relation to diabetic cheiroarthropathy, wherein the patient is requested to bring both the palmar surface of the hands together as at prayer. Prayer sign is said to be positive when patient is unable to bring both the palmar surface together completely and it indicates limited joint mobility. Limited joint mobility is secondary to nonenzymatic glycosylation of collagen and its deposition in the small joints of the hand [7].
2. Callosity on the forehead, from the Moslem style of praying several times a day, with the forehead touching the ground [8].
Preston’s Sign
Keratolysis or deciduous skin, a condition in which the whole skin is cast off like a snake in huge contiguous pieces. Also called Serpent sign. Deciduous skin can be defined best as continuous, periodic or seasonal shedding or peeling of the epidermal layer of the skin of more or less generalized distribution [9].
Price’s Sign
Press the thumb against the sternum and hold it there for a few seconds, then remove it quickly. If the blanched area does not turn pink in less than a second, this is an indication of early shock. Sign described by Philip Barton Price, American surgeon.
Primary Sign
Synonyme: chankroid. Induration, resulting in the site of entry of Treponema pallidum in syphilis [10].
Paronychia primarily from Mycobacteruim tuberculosis, contained within tissue sections [11].
Proud Flesh Sign
Exuberant granulation tissue around the opening of sinus track. A sign that signifies necrosis of bone is occurring in the depths of the track.
Prussic Sign
Giddiness, eyes staring, and teeth clenched. A sign of hydrocyanic acid poisoning [12].
Purple Foot Sign
Trench foot, mmersion foot was originally described in the military literature during World War I [13,14]. A characterized signs are pedal swelling, numbness, and pain.
In your work Atenstaedt described [15]:
“…. Trench foot appeared in the winter of 1914, characterized by pedal swelling, numbness, and pain. It was quickly recognized by military-medical authorities. There was little debate over whether it was frostbite or new condition, and it was quickly accepted as a specific disease. The major etiologies proposed were exposure, diet, and infection. The opinion emerged that it was caused by circulatory changes in the foot caused by cold, wet, and pressure. Predisposing factors included dietary inadequacy and fatigue. A number of labels were first given to the disease. However, the name “trench foot” was eventually officially sanctioned. Trench foot became a serious problem for the Allies, leading to 75 000 casualties in the British and 2000 in the American forces. Therapy for trench foot involved a number of conventional, tried-and-tested, and conservative methods. Some more innovative techniques were used. Amputation was only used as a last resort. Prevention involved general measures to improve the trench environment; modification of the footwear worn by the men; and the provision of greases to protect them from moisture. The medical reaction to this condition seems to have been relatively effective. The causation was identified, and prophylactic measures were introduced to fit this model; these seem to have been successful in reducing the prevalence of the condition by 1917-18…”
Purple Hair Sign
Hair becomes purplish brown when the scalp is treated with chrysarobin and then washed with an alkali soap [16].
Pseudo-acanthosis Nigricans Sign
Pseudo-acanthosis is a type of acanthosis nigricans that is seen in obese persons and is reversible on weight reduction [17].
Pseudo-acne Sign
Acneiform red papules along transverse nasal crease in preadolescent individuals. They are basically keratin granulomas derived from ruptured and inflamed milia. Due to their clinical similarity to acne, they have been named pseudo-acne [18].
Pseudo-ainhum Sign
Ainhum is the autoamputation of a digit, due to development of constricting bands around bilateral fifth toes, seen in underdeveloped countries of Africa (Fig. 3). In the remainder of the world, constricting bands that mimic ainhum are termed pseudo-ainhum. Causes of pseudo-ainhum are amniotic bands, constrictions associated with keratotic disorders, infections, and trauma [19].

Pseudo-bubo Sign
Seen in Donovanosis. Sub-cutaneous swellings in inguinal areas, which may break down to form typical granulomas, are known as pseudo-bubos since there is no lymphadenitis on microscopic examination [20].
Pseudo-chancre Redux Sign
This term is used to describe a solitary gumma of the penis at the site of the original chancre [21].
Pseudo-cowpox Sign
Milker’s nodule is otherwise known as pseudo-cowpox. It is a paravaccinia (parapox) virus infection seen in individuals in close contact with cattle, like milkers, veterinarians, and workers in meat industry. Cutaneous lesions can be one or several papulovesicles to bluish nodules, which may rupture to form ulcers with eschar. Cowpox is caused by the cowpox virus (orthopox) [22].
Pseudo-Darier Sign
When firmly stroked, fasciculation of the skin causes the appearance of goosebumps or cobblestones from the stimulation of aberrant arrector pili muscles – Smooth muscle hamartoma.
Pseudo-eccrine Chromhidrosis Sign
This refers to the development of colored sweat when surface compounds or molecules mix with sweat to produce pigment e.g. the formation of blue sweat in copper workers. Extrinsic dyes, paints, fungi, and chromogenic bacteria are other causes of pseudo-eccrine chromhidrosis [23].
Pseudo-elephantiasis Sign
Pseudo-elephantiasis is a condition, caused due to inflammation, edema or obstruction of lymphatics, triggered by non-filarial infections like donovanosis, lymphogranuloma venereum, syphilis, tuberculosis [24].
Pseudo-folliculitis Sign
Inflammatory papules resulting from re-entry of sharp tips of cut hair into the skin. Pseudo-folliculitis usually affects the beard area, when it is known as pseudo-folliculitis barbae [25].
Pseudo gall Sign
Eliminate certain parasitic pruritus such as scabies, difficult to diagnose in patients with strict hygiene, in the absence of specific signs (pseudo-bladder and groove), possibly by a testing treatment (Vulvar and anal pruritus) [26].
Pseudo-granuloma Inguinale Sign
It is a clinical variant of chancroid resembling granuloma inguinale (Donovanosis). Selective culture media isolates Hemophilus ducreyi from the penile ulcer, which clinically looks like granuloma inguinale [20].
Pseudo-Hutchinson’s Sign
Discoloration of the eponychium: Congenical nevus of the nail apparatus. (Fig. 4) [27].

Pseudo sign of Lesar Trelat
Inflammation of seborrheic keratosis caused by cytarabine: A pseudo sign of Leser-Trelat. A Leser-Trelat sign refers to multiple eruptive seborrheic keratosis, in the context of an internal malignancy [20].
Pseudo-monilethrix Sign
It is a hair shaft abnormality, where the hair shaft shows irregular, flattened, expanded areas that have an indented appearance, unlike monilethrix where the hair shafts have beaded appearance because of alternate zones of spindle-like thickening and thinning, placed at a regular intervals [28].
Pseudo-mycosis Sign
Botryomycosis is otherwise known as pseudo-mycosis. Cutaneous botryomycosis resembles a fungal infection but is actually a chronic, inflammatory response to bacterial infection. Staphylococcus aureus is the most commonly implicated bacteria, followed by Pseudomonas aeruginosa [29].
Pseudo-Nikolskiy Sign
The method and mechanism of elicitation is the same as for Nikolskiy sign but and can be elicited only on the involved or erythematous areas. The underlying mechanism here is the necrosis of epidermal cells and not acantholysis as in true Nikolskiy sign. This sign is positive in Stevens-Johnson syndrome, toxic epidermal necrolysis and in some cases of burns and bullous ichthyosiform erythroderma [20].
Pseudo-nits Sign
Peipilar keratin casts or hair casts or pseudo-nits are thin, elongated, firm, cylindrical concretions that encircle the hair shafts and can be easily dislodged, unlike true nits, which are oval, glistening, translucent, whitish lidded capsule attached to the side of the hair shaft by a firm chitinous sheath [20].
Pseudo-ochronosis Sign
Bluish-black macular pigmentation seen on the upper extremities of jewelry workers. Histopathologically, it is seen as localized argyria. The pigmentation simulates the typical pigmentation seen in endogenous ochronosis (alkaptonuria) [30].
Pseudo-paralysis of Parrot Sign
Originally described by Parrot, this pseudo-paralysis represents decreased movement of the extremity secondary to painful syphilitic periostitis [20].
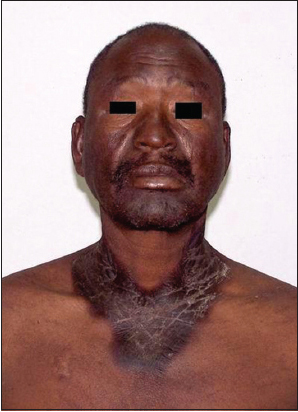
Pseudo-pseudoxanthoma Elasticum
It is a penicillamine-induced degenerative dermatosis, histopathologically characterized by abnormal elastic fibers in the dermis. Clinically, the patient develops multiple small yellowish papules on both sides of neck mimicking pseudo-xanthoma elasticum, after long term therapy with D-penicillamine [31].
Pseudo-rheumatoid Nodule Sign
Sub-cutaneous granuloma annulare is otherwise known as pseudo-rheumatoid nodule, because of their clinical resemblance to rheumatoid nodule. Lesions are nodular and predominantly occur on the scalp and pretibial regions [32].
Pseudo-scleroderma Sign
Pseudo-scleroderma refers to sclerosis of skin in conditions other than morphea or systemic sclerosis. This is seen in eosinophilic fasciitis, dermatomyositis, systemic lupus erythematosus, porphyria cutanea tarda, phenylketonuria or paraproteinemia [33].
Pseudo-syndactyly Sign
Pseudo-syndactyly is seen in dystrophic epidermolysis bullosa, autosomal-recessive forms, where repeated blistering with progressive scarring causes fusion of adjacent fingers and toes, thus giving rise to pseudo-syndactyly. True syndactyly is a congenital malformation, where there is failure of differentiation, in which the fingers fail to separate into individual appendages [34].
Pseudo-verrucous Papules Sign or Pseudo-verrucous Papules Nodules Sign
Pseudo-verrucous papules and nodules occur in the diaper and perineal areas in patients, of any age, with a predisposition to prolonged wetness. Children who wear diapers due to chronic urinary incontinence are prone to this type of dermatitis [35].
Pseudo-xanthoma Elasticum Sign
Pseudo-xanthoma elasticum is an inherited disorder characterized by generalized fragmentation and progressive mineralization of the elastic fibers in various tissues, involving the dermis (in flexural sites), eye (angioid streak and retinal defects), and cardiovascular system (hypertension and vascular disease). Cutaneous lesions are small, yellowish papules occur in a linear or reticular pattern, commonly involving areas like the sides of neck, axillae, groins, and perineum [36].
Punshi’s Sign
In young women and girls having from vitiligo the original white color of vitiligo macules turns to red-pink during menstruation and after the menstruation, it turns to the original colour [37]. Sign described in 1970.
Satish Kashiram Punshi
Dermatologist from India (Fig. 5). He was born in the year 1939. He is a well known writer, a thinker, philosopher, a social worker and a dermatologist of international repute, all rolled up in one. He is one of the most famous author of medical books on the topic Leucoderma. He is one who is pioneer for introducing placental extract therapy in Vitiligo (Leucoderma) and winner of prestigious International Lions award for Leprosy eradication. Dr. S. K. Punshi’s work on Leucoderma is quoted in various books and Journals of Dermatology. He completed his Medical Dgree M.B.B.S. from the Indore and went on to get D.D.V. from Mumbai, his academic qualification also includes F.I.M.S., F.D.S. (London). Though being engaged with writing of Medical books and serving the patients of skin diseases, he being awoken soul always find time to spend for the social works and thinks about the development of deprived section of society. During his long illustrated social life at Amravati city Dr. Punshi is active with many social organizations like Amravati Junior Chamber [Ex. Vice President], Loins Club of Amravati Central [Ex. President] along with being the life member of Red Cross Society, Sangit Kala Upasak Mandal, Cancer relief society, Vivekananda Ashram Society and many more. He also attended many national and international conferences and at few he was the Guest Speaker. In the Sindhi literature, Dr.Punshi is the famous personality for being the Author of Biography of Famous sindhi Saint Bhagat Kanwar Ram and spiritual master Sant Satramdas Sahib Ji. His many articles are published in Hindvasi (Sindhi), Illustrated weekly of India, Hindustan, Times of India, Hitvada and Nagpur times etc. Divine knowledge (A scientific approach to the study of Geeta), Biography of Dr. A. V. Mudliyar, Sindh darshan and Saint Kashiram- Roohani Rahbar are the some of other books written by him.
Dr. Punshi with all his achievements remains simple, solumn, sober, without much pomp and show and fanfare. He believes in God says “All is God’s will; man is just an instrument in the hands of God”.
He has more of Humanistic and Holistic approach to life”. He is a humble servant of humanity. He has lived his life for the cause and service of others. Nothing did for the self accept suffering.
Author Medical Books: 1. Vitiligo – Diagnosis and treatment; 2. Vitiligo and placental extract; 3. Vitiligo – quarterly medical review; 4. A Hand books of Scabies; 5. A Hand books of Leprosy; 6. Dermatology for general practitioners; 7. Colour Atlas of Vitiligo (Jaypee Brothers); 8. Diagnosis & Management of Dermatology made easy. (Jaypee Brothers).
Awards: 1. All India Award by skin institute Delhi in 1977 for research on use of placental extract in Leucoderma; 2. ‘ Ambady Oration’ award I 1986; 3. International Lions award for Leprosy eradication; 4. Lifetime achievement award I.A.D.V.L- Maharashtra state 2010; 5. Saint Kanwaram award; 6. Proffesor Hasanand memorial award.
“One who works in devotion, who is a pure soul, and who controls his mind and senses is dear to everyone, and everyone is dear to him. Though always working, such a man is never entangled.”
Pup-tent Sign
It is seen in nail lichen planus, in which the nail splits and elevates longitudinally with downward angle of lateral nail edge [38,39].
Puumala Sign
Rapid fever, kidney failure, severe back pain, and bleeding rash which progresses to death in 15 percent of victims. Caused by a zoonotic hantaviral infectious process known as hemorrhagic fever with renal syndrome disease [40].
REFERENCES
1. Shah A, Lakhani R, Panesar J, Rhinophyma–a patient case studyJ Vis Commun Med 2013; 36: 128-31.
2. de Faria MT, Calderwood MS, Athanazio DA, McBride AJ, Hartskeerl RA, Pereira MM, Ko AI, Carriage of Leptospira interrogans among domestic rats from an urban setting highly endemic for leptospirosis in BrazilActa Trop 2008; 108: 1-5.
3. Brzezinski P, Sinjab AT, Masferrer E, Gopie P, Naraysingh V, Yamamoto T, Dermatology Eponyms – sign – Lexicon (G)Our Dermatol Online 2012; 3: 243-57.
4. Brzeziński P, Passarini B, Nogueira A, Dermatology eponyms – phenomen / sign – dictionary (C)N Dermatol Online 2011; 2: 81-100.
5. Barro/Traoré F, Diallo B, Tapsoba P, Andonaba J-B, Kéré M, Niamba P, La [Pellagra: epidemiological and clinical features in the western region of Burkina Fasoo]Our Dermatol Online 2013; 4: 479-83.
6. de Souza CA, Santos Ada C, Santos Lda C, Carneiro AL, Hereditary tylosis syndrome and esophagus cancerAn Bras Dermatol 2009; 84: 527-9.
7. Papadakis G, Zampelis T, Michalopoulou M, Konstantopoulos K, Rosenberg T, Chatzipanagiotou S, Prayer Marks in Immigrants from Bangladesh with Diabetes Who Live in GreeceJ Immigr Minor Health 2015; Mar18[Epub ahead of print]
8. Raman PG, Jhavar D, Prayer sign. Diabetic cheiroarthropathyJ Assoc Physicians India 2003; 51: 1077-
9. Bechet PE, Deciduous skinArch Derm Syphilol 1938; 37: 267-1.
10. Gu X, Guan Z, Chai Z, Zhou P, Unilateral mydriasis as the primary sign of neurosyphilisInfection 2014; 42: 215-7.
11. Witthaut J, Möhlen S, [Chronic paronychia and synovialitis of extensor tendons due to Mycobacterium marinum. Is diagnosis or treatment the problem?]Handchir Mikrochir Plast Chir 2000; 32: 343-6.
12. Schapira K, Kessler BD, Howland MA, Su M, Intravenous cobinamide versus hydroxocobalamin for acute treatment of severe cyanide poisoning in a swine (Sus scrofa) modelAnn Emerg Med 2015; 65: 234-5.
13. Brzezinski P, Comment: The selection of the types of shoes and its impact on the skin of the feetOur Dermatol Online 2012; 3: 224-5.
14. Holden LG, Nicholson G, Trench feetJ R Army Med Corps 2014; 160: Suppl 1i36-7.
15. Atenstaedt RL, Trench foot: the medical response in the first World War 1914-18Wilderness Environ Med 2006; 17: 282-9.
16. Giovanoli-Jakubczak T, Greenwood MR, Smith JC, Clarkson TW, Determination of total and inorganic mercury in hair by flameless atomic absorption, and of methylmercury by gas chromatographyClin Chem 1974; 20: 222-9.
17. von Schnakenburg C, Enke B, Jürgens K, Offner G, [Pseudo-Acanthosis nigricans in a 12 year old boy after kidney transplantation]Klin Padiatr 2001; 213: 288-9.
18. Grando LR, Leite OG, Cestari TF, Pseudo-acne fulminans associated with oral isotretinoinAn Bras Dermatol 2014; 89: 657-9.
19. Castori M, Valiante M, Ritelli M, Preziosi N, Colombi M, Paradisi M, Palmoplantar keratoderma, pseudo-ainhum, and universal atrichia: A new patient and review of the palmoplantar keratoderma-congenital alopecia syndromeAm J Med Genet A 2010; 152A: 2043-7.
20. Ghosh S, Jain VK, “Pseudo” Nomenclature in Dermatology: What’s in a Name?Indian J Dermatol 2013; 58: 369-76.
21. Lanigan-O’Keeffe FM, Pseudo-chancre ReduxBr Med J 1965; 2: 212-
22. Giesecke WH, Theodorides A, Els HJ, Pseudo-cowpox (paravaccinia) in dairy cowsJ S Afr Vet Med Assoc 1971; 42: 193-4.
23. Gaffney DC, Cooper HL, Coloured sweat in two brothers: First report of familial chromhidrosisAustralas J Dermatol 2015; Mar5doi:10.1111/ajd.12262[Epub ahead of print]
24. Silva BB, Costa PV, Dias HK, Batista SM, [Vulvar donovanosis as pseudo-elephantiasis]Rev Assoc Med Bras 2006; 52: 11-
25. Cirincione VJ, The treatment of pseudo-folliculitisJ Med Assoc Ga 1962; 51: 388-9.
26. Lerch M, Peteja M, Ihnát P, Lerchová I, Zatloukal A, Zonča P, [Pruritus ani]Rozhl Chir 2015; 94: 269-75.
27. Sawada M, Ishizaki S, Kobayashi K, Dekio I, Tanaka M, Longterm digital monitoring in the diagnosis and management of congenital nevi of the nail apparatus showing pseudo-Hutchinson’s signDermatol Pract Concept 2014; 4: 37-40.
28. Phillips BB, Bayles MA, Grace HJ, Pseudo-monilethrix: further family studiesHumangenetik 1974; 25: 331-7.
29. Coelho WS, Diniz LM, Souza Filho JB, Cutaneous botryomycosis – case reportAn Bras Dermatol 2009; 84: 396-9.
30. Devins KM, Mogavero HS, JrHelm TN, Localized argyria with pseudo-ochronosisCutis 2015; 95: 20-29-31
31. Ibáñez-Samaniego L, Ochoa-Palominos A, Catalina-Rodríguez MV, Salcedo-Plaza M, Clemente-Ricote G, Penicillamine induced pseudo-pseudoxanthoma elasticum in a patient with Wilson’s disease, which role plays the hepatologist?Rev Esp Enferm Dig 2015; 107: 190-1.
32. Sharma A, Shortt A, Meligonis G, Rose GE, Periocular pseudo-rheumatoid nodules commonly affect the orbital rimOrbit 2008; 27: 341-4.
33. Haustein UF, Scleroderma and pseudo-scleroderma: uncommon presentationsClin Dermatol 2005; 23: 480-90.
34. Ezzine Sebaï N, Trojjet S, Khaled A, Zekri S, Fazaa B, Jaafoura MH, [Kindler syndrome: three cases reports in three siblings]Ann Dermatol Venereol 2007; 134: 774-8.
35. Maruani A, Lorette G, Barbarot S, Potier A, Bessis D, Hasselmann C, Re-emergence of papulonodular napkin dermatitis with use of reusable diapers: report of 5 casesEur J Dermatol 2013; 23: 246-9.
36. Lamb CM, Johns RA, Gallagher PJ, Odurny A, Shearman CP, A case of pseudo-xanthoma elasticum presenting with ischaemic claudicationEur J Vasc Endovasc Surg 2012; 43: 478-9.
37. Punshi SK, Linear VitiligoIndian J Dermatol Venerol Leprol 1975; 41: 240-
38. Puri N, Puri A, A study on topical calcium dobesilate for the treatment of limited plaque psoriasisOur Dermatol Online 2013; 4: 290-3.
39. Chang P, Dorsal Ungual PterygiumOur Dermatol Online 2012; 3: 57-60.
40. Manigold T, Vial P, Human hantavirus infections: epidemiology, clinical features, pathogenesis and immunologySwiss Med Wkly 2014; 144: w13937-
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.