Manifestations and intensity of indirect self-destructiveness in patients with psoriasis vulgaris
Wojciech Bienias, Andrzej Kaszuba
Department of Dermatology, Pediatric Dermatology and Dermatological Oncology, Medical University of Lodz, Lodz, Poland
ABSTRACT
Introduction: Psoriasis is a chronic systemic disease which often significantly reduces the quality of life in extreme situations can provide to severe depression and even suicide. Indirect self-destructiveness is a generalized trend of behavior consisting of taking steps to increase the likelihood of negative and reduce the likelihood of positive consequences for the entity within a general manifestations such as transgression of norms and risk, addictions, poor health maintenance, personal and social neglect, lack of planfulness, helplessness and passiveness. Polish and world literature has no publications on indirect self-destructiveness in psoriasis nor in any skin diseases. The main aim of this study was to investigate the intensity and symptoms of indirect self-destructiveness in population of patients with psoriasis vulgaris
Material and methods: The material consisted of 82 patients with psoriasis vulgaris hospitalized in the Department of Dermatology, Pediatric Dermatology and Oncology in 2013-2014. For the achievement of the objectives of the research socio-demographic questionnaire (own authorship) and Indirect Chronic Self-Destructiveness Scale by Kelley in Polish adaptation of Suchańska (version for men and women – each containing 52 issues) was used.
Results: The results showed that in a population of people with psoriasis overall severity of indirect self-destructiveness was in the lower range of the average results. The dominant class of indirect self-destructiveness was helplessness and passivity that preceded the poor health maintenance and lack of planning.
Conclusions: The results will enrich the existing knowledge about the harmful conduct of psoriasis and a better approach to the patient.
Key words: Psoriasis; Indirect self-destructiveness; Symptoms; Stress; Addictions
INTRODUCTION
Psoriasis Vulgaris and its Psychosocial Aspects
Psoriasis is a common chronic inflammatory disease, whose main manifestation are skin lesions such as hyperkeratotic papules and plaques covered with a layer of scales. The disease affects approximately 2-3% of the world’s population. In addition to skin psoriasis also affects joints and cardiovascular system [1–5].
Psoriasis significantly impairs the quality of life of people affected by it, and the degree of reduction in quality of life is similar to that of diabetes, cancers or acute myocardial infarction [6–11].
Psoriasis also contribute to the formation of secondary changes in the psyche of a person suffering from this condition, they are responsible for depressed mood, depression, anxiety, the social isolation and withdrawal. Severe itching that often accompanies psoriasis very significantly promotes sleep disorders, especially an insomnia. About 5% of patients with the most severe forms of psoriasis (eg. erythrodermic psoriasis) attempt suicide. Psoriasis also affects social functioning, is primarily the cause of stigmatization of people suffering from this disease, it contributes to worse functioning in the family and at work. It has been proven also that the fact of having psoriasis favors addictions (smoking, drinking, drug use) that may be a mechanism of escape from a difficult situation resulting from the disease.
People with psoriasis often statistically don’t join in the formal and informal relationships and divorce more often. Finally, the presence of psoriasis impairs the sexual sphere [12–29].
Susceptibility to the development of psoriasis is genetically conditioned, and the inheritance of susceptibility is poligenic. In addition to genes the occurrence or exacerbation of psoriasis is also influenced by environmental factors, among which the most important are stress, addictions (smoking and alcohol abuse) and infections, injuries or certain drugs [1–5].
In this situation stress and addictions are often both one of the causes and main effect of psoriasis.
Indirect Self-Destructiveness- Characteristics of the Concept and its Relationship with Psoriasis
Indirect self-destructiveness, also called chronic, hidden or latent is defined most often as a tendency to engage in behavior that increase the likelihood of negative and reduce the likelihood of positive consequences for the entity [30–33].
Indirect self-destructiveness is often called “suicidal lifestyle.” What differentiates indirect self-destructiveness from its direct form (which include suicide and self-mutilations) is mainly the result of the action which is unnecessary and away in time.
The main manifestations of indirect self-destructiveness include: intentional suffering and defeat, helplessness, passivity, social and health neglects, addictions, transgression and violation of social norms and heedlessness and inability to plan and succumbing to temptation. According with Suchańska and Kelley we can distinguish 5 classes of indirect self-destructiveness designated A1-A5 (A1- transgression of norms and risk, addictions, A2-poor health maintenance, A3 – personal and social neglect, A4- lack of planfulness and A5 – helplessness and passiveness in the face of the problems). These classes are not separate entities but mutually overlapping, so that it is often difficult to classify the exact manifestation of a particular class [30–37].
After characterization of psoriasis vulgaris and indirect self-destructiveness it is well obvious that although this notions are seemingly quite far apart, they have several common aspects.
Addictions and neglect of health are manifestations of indirect self-destructiveness which are certainly associated with psoriasis, as evidenced by numerous publications devoted to this subject [13,15,17,19].
Indirect self-destructiveness determine unfavorable lifestyle, a lifestyle is according to the paradigm of Lalonde the major determinant of human health, and also the only one for which the subject has any impact thus linking frequent dermatological disease- psoriasis with indirect self-destructiveness, in the absence of any existing so far publications this topic seems to be well reasoned and practical at the same time [38].
The aim of the study was to determine the intensity and major symptoms of indirect self-destructiveness in the population of patients with psoriasis.
MATERIALS AND METHODS
The study included 82 adult patients with psoriasis vulgaris hospitalized in the Department of Dermatology, Pediatric Dermatology and Oncology in Lodz in 2013-2014 (27 women and 55 men, mean age 46.6 years). The study excluded patients suffering from other serious chronic diseases, especially neurological and psychiatric diseases. The subjects completed a questionnaire, patients demographic and composed of 52 sentences questionnaire investigating indirect self-destructiveness in adaptation of Suchańska, separate version for men and women. At each of the 52 statements patient chose an option answers – from A (strongly agree) on E (strongly disagree), on the basis of assigned each response scores determined the overall rate of intensity of indirect self-destructiveness (minimum score 52 points, the maximum 260 points) in turn, each related to one of 5 classes of indirect self-destructiveness, allowing also to define the dominant symptoms of a patient. The study was approved by the Bioethics Committee and participation in the survey was voluntary.
All calculation and graphs were made using Statistica 11PL and Ms Office 2007.
RESULTS
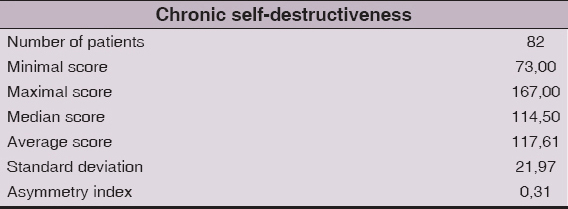
The average score of indirect self-destructiveness in the population studied was 117.61 ± 21.97 (median = 114.5).
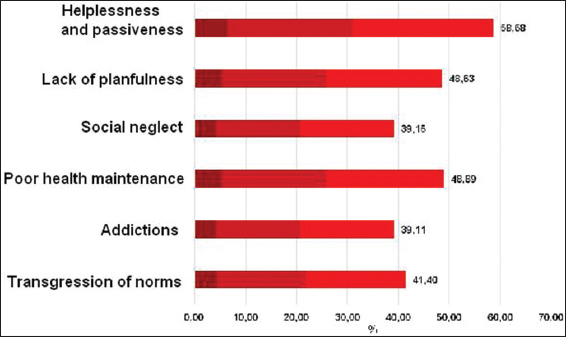
The average score of class A1 “Transgression risk” of indirect self-destructiveness was in the examined population 41.40 ± 10.39 (median = 40.00).
The average score of class A1a “Addictions” of indirect self-destructiveness was in the examined population 39.11 ± 17.36 (median = 36.67).
The average score of class A2 – “Poor health maintenance” of indirect self-destructiveness was in the examined population 48.89 ± 12.66 (median = 47.50).
The average score of class A3 “Social neglect” of indirect self-destructiveness was in the examined population 39.15 ± 9.40 (median = 39.09).
The average score of class A4 “ lack of planfulness” of indirect self-destructiveness was in the examined population 48.63 ± 10.59 (median = 48.89).
The average score of class A5 “helplessness and passivity” of indirect self-destructiveness was in the examined population, 58.68 ± 13.65 (median = 60.00). The data shown in Fig. 1 and Table 1.
DISCUSSION
The average score of indirect self-destructiveness in patients with psoriasis vulgaris was in the lower range of average results.
The most expressed class of indirect self-destructiveness in patients with psoriasis was A5 “Helplessness and passivity” in second place of intensity there were almost simultaneously class A2” Poor health maintenance” and class A4 “ Lack of planfulnes”. The less expressed class of indirect self-destructiveness was in this population class A1 “Transgression of norms and risk” and its subclass A1a “Addiction”.
As we can see passive forms of indirect self-destructiveness strongly dominate in patients with psoriasis vulgaris over its active forms.
As it turns out, the biggest problem of people with psoriasis is their overwhelming helplessness, passivity and resignation. People with psoriasis, especially with its most severe forms are resigned, don’t believe in the therapeutic success, don’t believe in success in life are pessimistic for the future, have a great sense of injustice in the world and have feelings of lack of control.
This passivity and helplessness can be a cause of a poor health maintenance, with a predominance of non adherence to medical recommendations and leaving the check-ups.
Thus smoking and drinking alcohol is not a leading problem in population of psoriatic patients and it seems that it can be an ineffective and desperate form of escaping from the psychosocial problems caused by psoriasis.
CONCLUSIONS
The conclusions from this study allow to optimize the approach to a patient with psoriasis. In everyday contact with the patient dermatologist must first activate and motivate a person, strengthen his motivation and educate and explain that it is possible to achieve the remission with the appropriate involvement of the patient and his positive thinking so needed in the therapeutic process. The attitude of forbidding of smoking and drinking alcohol is then ineffective and destroys the therapeutic relationship as well as may contribute to even greater helplessness.
Chronic self-destructiveness is a quite enigmatic psychological issue that in dermatology has been never investigated or reported. Thus, it is the first study integrating chronic self-destructiveness with skin disease. Until now indirect self-destructiveness was studied in field of psychiatry in patients with schizophrenia in people after suicide attempts and in drug addicts [39–41].
The relationship of chronic self-destructiveness with psychiatry seems obvious, however, as shown in this work, because of bilateral interaction between the skin and the psyche, the study of indirect self-destructiveness in psoriasis has its strong justification and practical implications.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
REFERENCES
1. Jabłońska S, Majewski S, Choroby skóry i choroby przenoszone drogą płciową 2008; Warszawa: PZWL;
2. Sterry W, Paus R, Burgdorf W, Dermatologia 2009; Lublin: Wydawnictwo Czelej;
3. Braun-Falco Burgdorf WHC, Plewig G, Wolff HH, Landthaler M, Dermatologia, tom I 2010; Lublin: Wydawnictwo Czelej;
4. Kaszuba A, Adamski Z, Leksykon Dermatologiczny, tom I 2011; Lublin: Czelej;
5. Moreno-Gimenez JC, Jimenez-Puya R, Galan-Gutierrez M, Comorbidities in psoriasisActas Dermosifilogr 2010; 101: 55-61.
6. Gaikwad R, Deshpande S, Raje S, Dhamdhere DH, Ghate MR, Evaluation of functional impairment in psoriasisIndian J Dermatol Venerol Leprol 2006; 72: 36-40.
7. Choi J, Koo JYM, Quality of life issues in psoriasisJ Am Acad Dermatol 2003; 49: 557-61.
8. Aghaei S, Moradi A, Ardekani GS, Impact of psoriasis on quality of life in Iran 2009; 75: 220-
9. Kanikowska A, Kramer L, Pawlaczyk M, Quality of life in Polish patients with psoriasisJ Eur Acad Dermatol Venerol 2009; 23: 92-3.
10. Hariram P, Mosam A, Aboobaker J, Esterhuizen T, Quality of life in psoriasis patients in KwaZulu NatalSouth Africa Indian J Dermatol Venereol Leprol 2011; 77: 333-4.
11. Lin TY, See LC, Shen YM, Liang CY, Chang HN, Lin YK, Quality of life in patients with psoriasis in northern TaiwanChang Gung Med J 2011; 34: 186-96.
12. Devrmici-Ozguven H, Kundakci N, Kumbasar H, Boyvat A, The depression, anxiety, life satisfaction and affective expression level in psoriasis patientJEADV 2000; 14: 267-1.
13. Basavaraj KH, Navya MA, Rashmi R, Stress and quality of life in psoriasis: an updateInt J Dermatol 2011; 50: 783-92.
14. Gupta MA, Gupta AK, Psychiatric and Psychological Co-Morbidity in patients with dermatologic disordersAm J Clin Dermatol 2003; 4: 833-42.
15. Linder D, Forchetti G, Psoriasis and psyche- what’s new? What is clinically relevant?Acta Dermatovenerol Croat 2009; 17: 198-203.
16. O’Leary CJ, Creamer D, Higgins E, Weinman J, Perceived stress, stress attributions and psychological distress in psoriasisJ Psych Res 2004; 57: 465-71.
17. Hayes J, Koo J, Psoriasis: depression, anxiety, smoking and drinking habitsDermatol Ther 2010; 23: 174-80.
18. Van Voorhees AS, Fried R, Depression and quality of life in psoriasisPostgrad Med 2009; 121: 154-61.
19. Cornish L, Kleinstein S, Living with psoriasisDermatol Nurs 2008; 20: 478-92.
20. Daus L, Give them a hand: patients with hand and foot psoriasis require special attentionDermatol Nurs 2008; 20: 291-3.
21. Ludwig MW, Oliveira Mda S, Muller MC, Moraes JF, Quality of life and site of the lesion in dermatological patientsAn Bras Dermatol 2009; 84: 143-50.
22. Reich H, Hrehorów E, Szepietowski JC, Pruritus is an important factor negatively influencing the well-being of psoriatic patientsActa Derm Venerol 2010; 90: 257-63.
23. Gowda S, Goldblum OM, McCall WV, Feldman SR, Factors affecting sleep quality in patients with psoriasisJ Am Acad Dermatol 2010; 63: 114-23.
24. Basra M.K.A, Finlay A.Y, Family impact of skin diseases: the Greater Patient conceptBr J Dermatol 2007; 156: 929-37.
25. Jafferani M, Psychodermatology: A guide to Understanding common psychocutaneus disordersPrim Care Companion J Clin Psychitry 2007; 9: 203-13.
26. Perrott SB, Murray AH, Lowe J, Mathieson CM, The psychosocial impact of psoriasis: physical severity, quality of life and stigmatizationPhysiol Behav 2000; 70: 567-71.
27. Barankin B, DeKoven J, Psychosocial effect of common skin diseasesCan Fam Physician 2002; 48: 712-6.
28. Boulinguez S, Psychosocial reverberations of psoriasisAnn Dermatol Venerol 2010; 137: 16-27.
29. Meeuwis KA, de Hullu JA, van de Nieuwenhof HPI, Evers AWM, Massuger LFAG, van de Kerkhof PCM, Quality of life and sexual health in patients with genital psoriasisBr J Dermatol 2011; 164: 1247-55.
30. Kelley K, Chronic self-destructiveness conceptualization measurement and initial validation of the constructMotivation and emotion 1985; 9: 135-
31. Kelley K, Cheung F, Rodriguez C, Singh R, Chronic self-destructiveness and Locus of Control in Cross Cultural PerspectiveJ Soc Psychol 1986; 126: 573-7.
32. Kelly DB, Rollings AL, Harmon JG, Chronic self-destructiveness, hopelesseness, and risk-taking in college studentsPsychol. Rep 2005; 96: 620-4.
33. Suchańska A, Behawioralne wskaźniki po&#średniej autodestruktywno&#ści a styl wyja&#śniania zdarzeńCzasopismo Psychologiczne 1995; 1: 1-2.
34. Suchańska A, Przejawy i uwarunkowania psychologiczne po&#średniej autodestruktywno&#ści 1998; Poznań: Wydawnictwo Naukowe UAM;
35. Suchańska A, Po&#średnia autodestruktywnołć–operacjonalizacjai pomiar zjawiska 1992; Poznań: Raport z badańfinasowanych z grantu wewnętrznego Instytutu Psychologii UAM;
36. Suchańska A, Problem intencjonalno&#ści zachowańautodestruktywnych. W: Elementy psychologii klinicznej, tom V 1998; Poznań: Wydawnictwo Naukowe UAM;
37. Suchańska A, Ukryty wymiar samozniszczenia. W: Elementy psychologii klinicznej 2005; Poznań: Wydawnictwo UAM;
38. Lalonde M, A New Perspective on the Canadians. in Working Document 1974; Ontario: Minister of National Health and Welfare;
39. Tsirigotis K, Gruszczyński W, Zachowania autodestrukcyjne u chorych zrozpoznaniem schizofreniiSuicydologia 2008; 4: 29-36.
40. Tsirigotis K, Gruszczyński W, Kruszyna M, Autodestruktywnołćpo&#średnia u osób popróbach samobójczychSuicydologia 2008; 4: 57-62.
41. Tsirigotis K, Gruszczyński W, Kruszyna M, Tsirigotis-Wołoszczak M, Autodestruktywnołćpo&#średnia u osób uzależnionych od narkotykówAlkoholizm I Narkomania 2009; 2: 119-28.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.