Blaschkoid lichen planus: A rare presentation of a common disease
Mohammad Adil, Syed Suhail Amin, Tasleem Arif
Postgraduate Department of Dermatology, STDs and Leprosy, Jawaharlal Nehru Medical College (JNMC), Aligarh Muslim University (AMU), Aligarh, India
Sir,
Lichen planus (LP) is a common dermatological disease that classically presents with purple, polygonal, pruritic, flat topped papules on the skin, but can also involve mucosae and nails [1]. Many morphological variants of LP have been described. The linear variant following the lines of Blaschko is an extremely rare entity and must be differentiated from the commoner linear LP as a result of koebnerization due to trauma and zosteriform LP [2]. The rarity of this pattern of the LP inspired us to present this case.
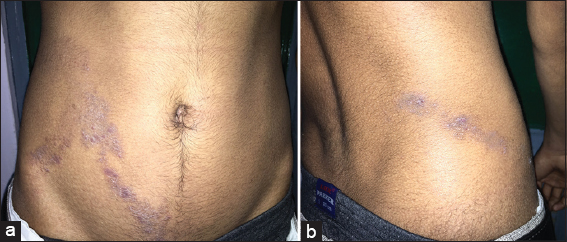
A 17 year old healthy male presented with multiple purple colored lesions on the right side of his lower trunk which he had noticed one month back. These lesions were associated with itching. The patient did not give any history of trauma, topical applications of any medications or any recent medical or surgical illness. On examination, there were multiple, discrete, violaceous, closely set, flat topped, 2-5 mm papules, strictly unilaterally on the right side of the body in a distinct S- shaped pattern arising from the right side of suprapubic region anteriorly to the lower back (Figs. 1a and 1b) along the lines of Blaschko. The scalp, hair, mucosae and nails were normal. Routine Laboratory investigations were unremarkable. Serology for HIV, Hepatitis B and C was negative. A 5 mm punch biopsy from the lesion was taken and sent for histopathological examination which showed hyperkeratosis, hypergranulosis, vacuolar degeneration of basal layer with a band like infiltrate at the dermo-epidermal junction along with melanin incontinence. Civatte bodies were identified in the epidermis. Based on the clinical and histopathological findings, a diagnosis of Blaschkoid LP was made and the patient was treated with topical corticosteroids (mometasone) and oral antihistamines. The patient responded favorably to treatment with resolution of the lesions and decreased itching.
Lichen planus is a fairly common dermatosis but unilateral LP along the lines of Blaschko has been rarely reported [3]. Lines of Blaschko are lines that represent the boundaries between normal and mutant skin due to mosaicism, and do not correspond to any vascular, lymphatic or neural structures [4]. These are V-shaped over the upper spine, S-shaped over the abdomen, U-shaped on the chest and upper arm and perpendicular on the extremities. Some congenital nevi and inflammatory diseases like psoriasis, vitiligo and LP may present in a nevoid form [5]. The linear variety of LP can simply be a result of Koebner’s phenomenon, segmental LP or zosteriform LP. It must also be differentiated with lichenoid epidermal nevus, lichen striatus, linear psoriasis or inflammatory linear verrucous epidermal nevus [6]. Happle (1996) was of the view that many cases of lichen planus along Blaschko lines are misdiagnosed as zosteriform lichen planus [7]. Blaschkoid LP is not associated with Hepatitis C or hepatocellular carcinomas while other varieties of linear LP can show such an association [8,9]. Typical pattern of distribution of the lesions with suggestive histopathology can help to settle the diagnosis.
Lichen planus in a Blaschkoid distribution is rare with only some case reports published till date [1–6,9,10]. A correct diagnosis of Blaschkoid LP and its differentiation from other causes of linear LP is important as unlike the former, the latter is associated with systemic diseases. The recognition of this rare entity will prevent unnecessary investigations, cutting monetary costs, saving time and will also prevent undue anxiety in the patient.
REFERENCES
1. Rather PA, Hassan I, Blaschkoid lichen planus in an adult Kashmiri male: A rare presentationOur Dermatol Online 2013; 4: 179-82.
2. Rehman SB, Bari AU, Mumtaz N, Unilateral Blaschkoid lichen planus involving the entire half of the body, a unique presentationDermatol Online J 2007; 13: 36-
3. Elghblawi E, Blaschkoian Lichen Planus in an Amazghi;A Rare Case ReportOpen Dermatol J 2014; 8: 45-50.
4. Gupta S, Gupta S, Thomas M, Mahendra A, Unilateral Lichen Planus along the lines of Blaschko: a rare clinical presentationActa Med Indones-Indones J Intern Med 2012; 44: 163-4.
5. Yayla D, Cakmak SK, Oguz ID, Gonul M, Ozhamam E, Colak A, Two cases of unilateral lichen planus following the lines of BlasvhkoAnn Dermatol 2014; 26: 636-8.
6. Kavoussi H, Ramazani M, Salimi E, Lichen planus along with Blaschko lines “Blaschkoian lichen planus”J Pak Assoc Dermatol 2013; 23: 153-8.
7. Happle R, “Zosteriform” lichen planus: is it zosteriform?Dermatology 1996; 192: 385-6.
8. Jury C, Munro C, Linear lichen planus related to hepatitis C infection?Br J Dermatol 2000; 142: 836-7.
9. Lade NR, Saoji V, Singh AL, Blaschkoid Lichen Planus: not a Koebner’s phenomenonDermatol Online J 2013; 19: 17-
10. Klein HA, Krathen RA, Hsu S, Widespread blaschkoid lichen planusDermatol Online J 2006; 12: 17-
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.