Terra firma-forme dermatosis – a dirty dermatosis: report of two cases
Snehal Lunge, Supraja Chinthala
Department of Dermatology, Kle University, Jawaharlal Nehru Medical College, Belgaum, India
Submission: 02.11.2015; Acceptance: 28.01.2016
How to cite this article: Lunge S, Supraja C. Terra firma‑forme dermatosis – a dirty dermatosis: report of two cases. Our Dermatol Online. 2016;7(3):338‑340.
ABSTRACT
Terra firma-forme dermatosis is characterized by ‘dirty’ brown-grey cutaneous patches and plaques that can simply be eradicated by forceful swabbing with alcohol pads. The pathogenesis has been attributed to abnormal and delayed keratinization. Although affected patients present with typical lesions, the disorder is not well-known by physicians. From a clinical point of view, we lay emphasis on its unique expression and diagnosis/treatment. From a histological perspective, we highlight its resemblance to dermatosis neglecta and speculate on the role of ‘neglect’ in a patient with seemingly adequate hygiene. The role of urea containing emollients in the development of this disorder remains to be determined.
Key words: Dermatitis neglecta; Dermatosis neglecta; Terra firma.forme dermatosis
INTRODUCTION
Terra firma-forme dermatosis (TFFD) is a bizarre, acquired and idiopathic dermatosis [1]. The disorder was initially reported as a distinct entity by Duncan et al., in 1987. The Latin phrase terra–firma mean‘dry land’ and denotes a cutaneous discoloration resembling ‘dirt’ (hence the alternative name Duncan’s Dirty Dermatosis) [2].
CASE REPORTS
Case 1
A 26-year-old male presented with a 15 days history of persistent scaly pigmented patches on the nape of neck. Patient gives history of not taking bath for a period of 7 days.
Cutaneous examination revealed brown-grey patches on nape of neck (Fig. 1).

There were islands of normal skin within the patches. Initial tentative clinical diagnoses were terra firma-forme dermatosis, pomade crust, confluent and reticulated papillomatosis and acanthosis nigricans. A ‘wipe test’ with 70% ethyl alcohol accomplished clearance of lesions (Fig. 2).

Case 2
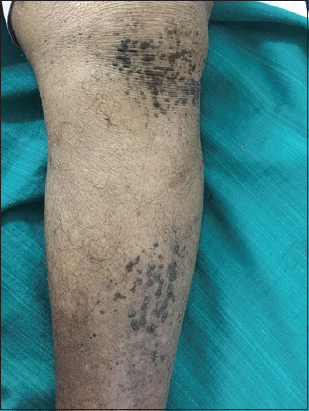
A 70-year-old male presented with a 25 to 30 days history of persistent scaly pigmented patches on the left leg. Patient gives history of admission in hospital for a systemic condition since 10 days.
Cutaneous examination revealed brown-grey patches on anterior surface of left leg (Fig. 3). There were islands of normal skin within the patches. A ‘wipe test’ with 70% ethyl alcohol accomplished clearance of lesions (Figs. 4 and 5).


DISCUSSION
TFFD is a recently described cutaneous pigmentation disorder. It is probably more prevalent than cited in the Literature. The disorder affects all age groups (age range: 3 months to 72 years) and both genders [1,3]. Clinically, TFFD is characterized by brown-grey, velvety, pigmented patches or plaques [2]. Involvement of the face, neck, trunk or ankles is usual, although unusual sites such as scalp, lips, chest, axilla, back, umbilical area, pubis, arms and legs have been reported [3–5]. The distribution may be localized, generalized or symmetrical. Rarely palpable verrucous or papillomatous plaques, reticulated patches and focal slight scaling have been observed [4].
Symptomatic cases are rare; however, TFFD is a cause of cosmetic concern [1].
The histopathological description encompasses prominent lamellar hyperkeratosis with focal areas of compact whorled orthokeratosis [1], papillomatosis, mild acanthosis and deposition of keratotic material within the valleys between the papilla [5]. There is no parakeratosis. Dermal inflammation is trivial [2,5]. Other findings with special stains include increased melanin content in the compact hyperkeratotic and basal areas of the epidermis (Fontana-Masson) [1], scattered keratin globules throughout stratum corneum (Toluidine blue) [1,5] and occasional yeast cells indicative of Pityrosporum (Periodic Acid Schiff) [5,6].
The diagnosis of TFFD is confirmed by forceful rubbing with a gauze pad immersed into 70% isopropyl alcohol [1,2] or ethyl alcohol. This diagnostic test prevents unnecessary laboratory work-up or biopsy [3]. In addition, it offers a magical and prompt therapeutic cure for the disorder [1,2]. A pink normal skin underneath is exposed after the wiping procedure [5]. Reappearance isunusual once the skin is devoid of ‘dirty’ appearance. Prophylactic weekly application of alcohol has been recommended for resistant or recurrent cases [1]. Patients should be reassured about the benign nature of TFFD and educated about the cleaning procedure.
Differential diagnosis includes acanthosis nigricans, confluent and reticulated papillomatosis, pityriasis versicolor, epidermal nevi, dirty neck syndrome of atopic dermatitis and dermatosis neglecta (DN) [1,3,5].
Most of these disorders can be excluded by alcohol swab test [1,3]. DN results from ‘neglect’, i.e. poor hygiene or inadequate skin cleansing [6]. TFFD is distinguished from DN arbitrarily by presence of adequate hygiene, absence of cornflake-like brownish scales and successful eradication of pigmentation with isopropyl alcohol in the former and effective clearance of lesions with soap and water in the latter [1, 2, 4–6].
However, isopropyl alcohol is operative in both disorders [1,5].
Histologically, DN is similar to TFFD, except for the absence of whorled hyperkeratosis in DN [1,5]. Nevertheless, the distinction between TFFD and DN is blurred and there seems to be a considerable clinical and histological overlap between the two disordeCONCLUSION
Dermatitis neglecta is an underreported, asymptomatic, but aesthetically bothersome dermatosis. Physicians need to be aware of this condition that can be clinically diagnosed and effectively and inexpensively treated.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Pavlović MD, Dragos V, Potocnik M, Adamic M, Terra firma-forme dermatosis in a childActa Dermatovenerol Alp Panonica Adriat 2008; 17: 41-2.
2. Guarneri C, Guarneri F, Cannavò SP, Terra firma-forme dermatosisInt J Dermatol 2008; 47: 482-4.
3. Berk DR, Terra firma-forme dermatosis: A retrospective review of 31 casesPediatr Dermatol 2012; 29: 297-300.
4. Berk DR, Bruckner AL, Terra firma-forme dermatosis in a 4-month-old girlPediatr Dermatol 2011; 28: 79-81.
5. Akkash L, Badran D, Al-Omari AQ, Terra Firma forme dermatosis. Case series and review of theliteratureJ Dtsch Dermatol Ges 2009; 7: 102-7.
6. Choudhary SV, Bisati S, Koley S, Dermatitis neglectaIndian J Dermatol Venereol Leprol 2011; 77: 62-3.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.