Ulcerative giant solitary trichoepithelioma of scalp: a rare presentation
Sundeep Chowdhry, Prashansa Jaiswal, Tapan Kumar Dhali
Department of Dermatology, Venereology and Leprology, Employees’ State Insurance Corporation Post Graduate Institute of Medical Sciences & Research, Basaidarapur, New Delhi-110015, India
ABSTRACT
Trichoepithelioma is a trichogenic tumor which arises from the inferior segment of hair follicle epithelium as hamartoma. Giant solitary trichoepithelioma (GST) has been defined as a solitary trichoepithelioma with a diameter greater than 2 cm. A 49-year-old female presented with a slow growing skin coloured swelling on the scalp of 8 years duration with recent history of ulceration and occasional bleeding. The local examination revealed a single well defined nodular swelling which was irregular in shape measuring approximately 2 × 2.5 cm. Histopathology from biopsy specimen revealed dark basaloid cells with scanty cytoplasm and darkly stained nucleus arranged in nests with horn cysts lacking high-grade atypia and mitosis, which was consistent with features of trichoepithelioma. Giant solitary trichoepithelioma of scalp is itself a rare entity and the present case is being reported with the additional component of ulceration in the lesion.
Key words: Trichogenic; Tumour; Scalp; Ulcerative; Trichoepithelioma
INTRODUCTION
Trichoepithelioma is a trichogenic tumor which arises from the inferior segment of hair follicle epithelium as hamartoma. Giant solitary trichoepithelioma is a distinct variant of trichoepithelioma. It has been defined as a solitary trichoepithelioma with a diameter greater than 2 cm [1]. It arises in elderly individuals and occurs mostly on the face, thigh and peri-anal region [2,3]. These features are in contrast to the conventional trichoepithelioma, which presents as multiple small translucent circumscribed papules of 2–4 mm in diameter, in children and young adult on the face. To the best of our knowledge no case of ulcerative giant solitary trichoepithelioma on scalp has been reported previously.
CASE REPORT
A 49-year-old female presented with a slow growing skin coloured swelling on the scalp of 8 years duration with recent onset of ulceration and occasional bleeding. The local examination revealed a single well defined nodular swelling which was irregular in shape measuring approximately 2 × 2.5 cm (Fig. 1). On palpation it was a firm, mildly tender with no increase of local temperature. The lesion bled on manipulation. There were no signs of infection at the site. Routine blood investigations were within normal limits. Touch impression smear showed few neutrophils with no organism. The general physical and systemic examinations did not reveal any abnormality. There were no palpable lymph nodes in head and neck area.

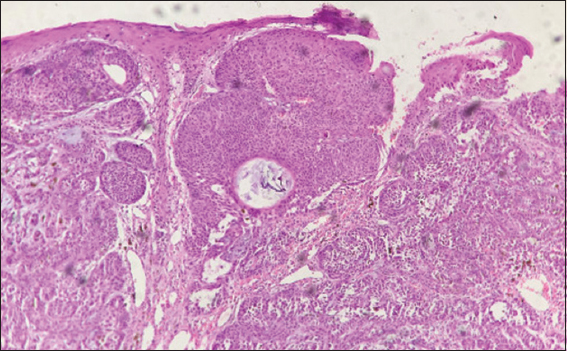
Histopathology from incisional biopsy specimen revealed dark basaloid cells with scanty cytoplasm and darkly stained nucleus arranged in nests with horn cysts, lacking high grade atypia and mitosis which was consistent with trichoepithelioma (Fig. 2). There was loss of epidermis suggesting ulcerative nature of the lesion (Fig. 3).

The patient was referred to the Department of Surgery for total excision and repair.
Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DISCUSSION
Trichoepithelioma (TE) was first described by Brooke in 1892 as Epithelioma Adenoides Cysticum [4]. Clinically, this tumor occurs either as a solitary lesion without familial association or as multiple lesions in multiple familial trichoepithelioma [5].
Since trichoepithelioma is inherited in an autosomal dominant fashion, males and females receive the gene equally. Because of lessened expressivity and penetrance in men, most patients are women [6]. A giant solitary trichoepithelioma is a distinct variant of trichoepithelioma that may have a predilection for the perianal region. At this site, this rare tumor must be distinguished from basal cell carcinoma of the perineum and from malignant basaloid (cloacogenic) carcinoma of the anal canal [2]. The mean age of the presentation is 60 years with a predilection for the older age group [7]. The majority of the GST has been subcutaneous but pedunculated [8] and ulcerated [6] appear as well.
The histopathology shows islands of uniform basaloid cells with scanty cytoplasm and darkly stained nucleus arranged in nests and adenoid pattern with epithelial islands. The epithelial islands may not connect to the overlying epidermis. The stroma may be fibromyxoid or fibrocellular [8,9]. Immature hair appears as keratinous cysts. These horn cysts are the characteristic features in most GST. They consist of fully keratinized center surrounded by basophilic cells that lack high-grade atypia and mitosis. The keratinization is abrupt and complete – the so called trichilemmal keratinization, which differentiates it from squamous cell carcinoma having gradual and incomplete keratinization in horn pearls [10]. GST presents as a pigmented lesion because of the increase activity of melanocytes or increased retention of pigment in the basal keratinocytes [11].
Treatment for multiple TEs include excision, electrodessication, dermabrasion, cryotherpy and radiotherapy, Argon, Carbon dioxide, erbium-YAG lasers. Surgical excision with or without flap is the standard treatment for most of GSTs. Radio-surgical ablation can be considered for cosmetic reasons when the tumor is situated over face. It helps in accurate removal of the tumor with minimal bleeding without destroying the underlying structures like cartilage. Malignant transformation into BCC after surgical excision requires adjuvant radiotherapy [12]. Recurrence and possible transformation into BCC necessitates patient follow up at regular intervals.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Teli B, Thrishuli PB, Santhosh R, Amar DN, Rajpurohit S, Giant solitary trichoepitheliomaSouth Asian J Cancer 2015; 4: 41-4.
2. Tatnall FM, Jones EW, Giant solitary trichoepitheliomas located in the perianal area: a report of three casesBr J Dermatol 1986; 115: 91-9.
3. Filho GB, Toppa NH, Miranda D, Matos MP, da Silva AL, Giant solitary trichoepitheliomaArch Dermatol 1984; 120: 797-8.
4. Anderson DE, Howell JB, Epithelioma adenoides cysticum: Genetic updateBr J Dermatol 1976; 95: 225-32.
5. Samaka RM, Bakry OA, Seleit I, Abdelwahed MM, Hassan RA, Multiple familial trichoepithelioma with malignant transformationIndian J Dermatol 2013; 58: 409-
6. Goya S, Mahajan NC, Garg M, Goyal S, Giant Solitary Nodular Trichoepithelioma: A Case Report and Review of LiteratureArch Clin Exp Surg 2012; 1: 58-60.
7. Colenje E, Burns T, Breathnach S, Cox N, Griffiths C, Tumours of the skin appendagesRook’s Textbook of Dermatology 2010; 3: 8th ed. West Sussex: Wiley-Blackwell Publishing;
8. Krishnamurthy J, Divya KN, The cytology of giant solitary trichoepitheliomasJ Cytol 2010; 27: 99-101.
9. Bedir R, Pergel A, Gucer H, Giant solitary trichoepithelioma: A Case reportDicle Med J 2013; 40: 137-40.
10. David E Elder, Rosalie Elenitsas, Adam I Rubin, Michal yloffreda, Jeffrey Miller O, Fred Miller III, Atlas and Synopsis of Lever’s Histopathology of the SkinChapter 6, Tumors and Cyst of epidermis and subcutis 2012; 3rd ed. Philadelphia: Lippincott-Raven; 364-
11. Rosai J, Rosai J, Skin – Tumors and tumorlike conditionsRosai and Ackerman’s Surgical Pathology 2004; St Louis: Mosby Elsevier; 176-
12. Martinez CA, Priolli DG, Piovesan H, Waisberg J, Nonsolitary giant perianal trichoepithelioma with malignant transformation into basal cell carcinoma: Report of a case and review of the literatureDis Colon Rectum 2004; 47: 773-7.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.