A black nodule on the temple
Yuka Inamura, Hiroo Hata, Keisuke Imafuku, Shinya Kitamrua, Hiroshi Shimizu
Department of Dermatology, Hokkaido University Graduate School of Medicine, North 15, West 7, Kita-ku, Sapporo 060-8638, Japan
Sir,
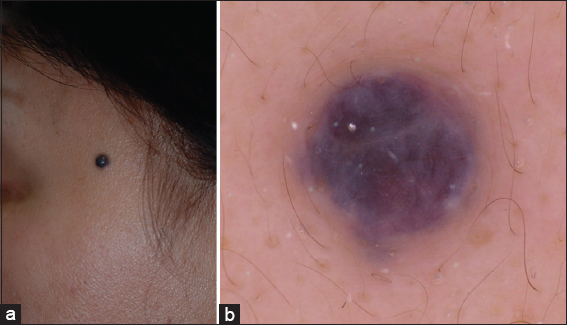
A 56-year-old female was referred to our hospital complaining of a nodule on the left temple. In the history-taking interview, she reported that the lesion had appeared 3 years before referral to our hospital as a tiny pinkish papule and had gradually enlarged. Physical examination found the nodule to be dark purple to black, well circumscribed, hemispherically raised and 5 × 5 mm in diameter (Fig. 1a). Dermoscopic examination revealed reddish-blue lacunae (Fig. 1b). We suspected hemangioma, venous malformation, apocrine hidrocystoma and basal cell carcinoma. We surgically removed the lesion for the correct diagnosis. In the histopathological findings, there were large vascular channels filled with abundant erythrocytes from the upper dermis to the subcutaneous tissues (Fig. 2a). There was no evidence of epidermal change. The vascular channels were lined by a single layer of endothelial cells or a thin wall of fibrous tissue (Fig. 2b).

Prior to the study, patient gave written consent to the examination and biopsy after having been informed about the procedure.
DIAGNOSIS
Venous lake
DISCUSSION
Venous lakes were first described by Bean and Walsh in 1956 [1].
They noted that venous lakes clinically present as soft, dark gray papules of a few millimeters in diameter with domed surface, often on the face, head and neck area, especially on the lower lips of elderly people. Histopathological study shows one to several dilated spaces with erythrocytes, and the lesions have very thin, fibrous walls. Usually, severe sun damage is evident in adjacent dermis. The pathogenesis of venous lake is still unclear. It is speculated that they venous lakes occur as a result of severe sun damage to collagen fibers that prevents venous dilation [2].
Venous lake clinically resembles angiokeratoma, apocrine hidrocystoma, basal cell carcinoma and malignant melanoma. It is comparatively easy to rule out basal cell carcinoma and malignant melanoma with dermoscopy; however, it is difficult to dermoscopically distinguish venous lake from other non-melanocytic tumors.
Venous lake often histopathologically mimics many kinds of vascular tumors. Angiokeratoma histopathologically demonstrates numerous dilated, thin-walled capillaries, mainly in the papillary dermis, whereas the epidermis presents acanthosis with elongated rete ridges and hyperkeratosis [3]. Epidermal changes and the location of the lesions are different from those in venous lake. Apocrine hidrocystoma is clinically similar to venous lake and histopathologically shows dilated ducts in the dermis; however, the walls of apocrine hidrocystomas are lined by rows of columnar cells and show decapitation secretion indicative of apocrine glands [4]. Apocrine hidrocystoma clinically resembles venous lake, although the pathological features are different.
Above all, we confirmed the diagnosis as venous lake. Venous lake usually appears on the lower lips, and if this lesion had been located on the lower lip, the diagnosis would have been easy. However, in this case, the black nodule was located on the left temple, so the diagnosis was more difficult.
Consent
The examination of the patient was conducted according to the Declaration of Helsinki principles.
REFERENCES
1. Bean WB, Walsh JR, Venous lakesArch Dermatol 1956; 74: 459-63.
2. Alcalay J, Sandbank M, The ultrastructure of cutaneous venous lakesInt J Dermatol 1987; 26: 645-6.
3. Schiller PI, Itin PH, Angiokeratomas: An updateDermatology 1996; 193: 275-82.
4. Smith JD, Chernosk Me, Apocrine hidrocystoma (cystadenoma)Arch Dermatol 1974; 109: 700-2.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.