Plaque with pearly raised borders on the forearm
Ruzeng Xue1, Manuel Valdebran2, David Terrero3, Bin Yang1
1Department of Dermatology, Guangdong Provincial Dermatology Hospital, Guangzhou, China, 2Ackerman Academy of Dermatopathology, New York, NY. USA[3] Research Department of the National Evangelical University Santo Domingo, Santo Domingo, Dominican Republic
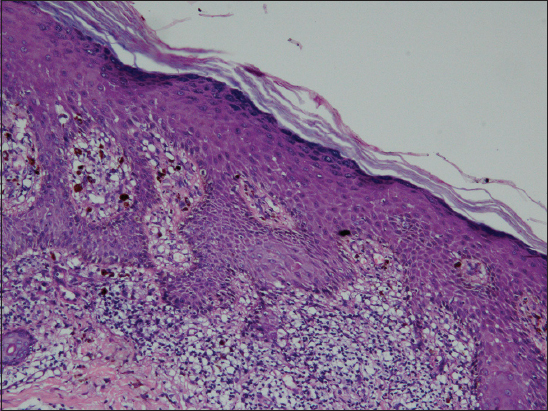
A 29-year-old male presented with an annular plaque on his arm for 7 months. Physical examination revealed 6 mm annular plaque with raised borders and a shiny stellate-purple center (Fig. 1). Dermoscopic evaluation revealed a ring of white spiked structurless areas at the periphery; an intense structurless steel purple area was observed at the center of the lesion (Fig. 2). Hystopathological examination showed a band-like infiltrate of lymphocytes, pigment incontinence, saw tooth rete ridges, hypergranulosis and hypekeratosis (Figs. 3 and 4).



Lichen planus annularis (LPA) is a rare variant of lichen planus; it might comprise less than 7% of LP cases [1,2]. Most frequently described locations include the genital and intertriginous areas, however, lesions on the trunk, extremities, eyelids and neck have been reported as well [3].
The pathogenesis of LPA has not been clearly elucidated nevertheless published data has revealed that the lichenoid tissue reaction might be triggered by a sequential activation of Langerhans cells, ultimately triggering the release of activated T cells which in turn migrate to the dermis and release several cytokines such as interleukins 1 and 2, and interferon gamma [4].
Interesting dermoscopic findings were the spiked white structurless areas in a circular disposition corresponding to Wickham striae; histopathologically it may correlate to the overall hyperplastic epidermis. Pigmentation at the center of the lesion is better appreciated dermoscopically showing a structurless steel purple area, corresponding histopathologically to areas of pigment incontinence in the papillary and reticular dermis. The black color of melanin is perceived as steel purple due to a tyndall effect. Long wavelengths are not reflected to the open air whereas shorter wavelengths are reflected and perceived by the eye as violet or blue [5].
In conclusion, interpretation of dermoscopic findings may help to infere histopathological changes to render an accurate diagnosis.
REFERENCES
1. Altman J, Perry HO, The variations and course of lichen planusArch Dermatol 196: 84179-91.
2. Voron D, MacVicar D, Annular lichen planusCutis 1973; 11: 635-6.
3. Reich HL, Nguyen JT, James WD, Annular lichen planus: a case series of 20 patientsJ Am Acad Dermatol 2004; 50: 595-9.
4. Yamanaka Y, Akiyama M, Shibaki A, Kikuchi T, Shimizu H, Annular lichen planus: study of the cellular mechanisms of annularityDermatology 2004; 208: 335-8.
5. Rootman DB, Lin JL, Goldberg R, Does the Tyndall effect describe the blue hue periodically observed in subdermal hyaluronic acid gel placement?Ophthal Plast Reconstr Surg 2014; 30: 524-7.
Notes
Source of Support: Nil,
Conflict of Interest: None declared.
Comments are closed.